

A single-center, cross-sectional study was designed to assess and compare objective and subjective quality of vision of patients intervened with penetrating keratoplasty (PK), deep anterior lamellar keratoplasty (DALK) and Descemet membrane endothelial keratoplasty (DMEK).
MethodsForty-six patients previously intervened with PK (22 eyes), DALK (7 eyes) and DMEK (17 eyes) were recruited. Visual evaluation included spherical and cylindrical refraction, distance corrected visual acuity (DCVA), photopic contrast sensitivity (CS), optical quality, measured with the HD Analyzer (objective scattering index [OSI], MTF cut-off and Strehl ratio), and ocular and corneal aberrometry, measured with the KR-1W Wavefront Analyzer.
ResultsStatistically significant between-group differences were found in age (p=0.006, DMEK patients were older) and time since surgery (p<0.001, longest time for PK patients). No statistically significant differences were found in DCVA between the techniques. Between-group differences were encountered in CS at 12 (p=0.007) and 18 (p<0.001) cycles per degree, with DMEK and DALK obtaining the best and worst outcomes, respectively. Differences in optical quality were found between the techniques (OSI, p=0.004; MTF cut-off, p=0.048; Strehl ratio p=0.022), with DMEK displaying the best outcomes. Highest and lowest values in ocular and corneal aberrations were for DALK and DMEK patients, respectively. Between-group differences were found in corneal astigmatism (p<0.001; −3.31±2.00 D in PK; −2.68±0.94 D in DALK; −1.09±0.62 D in DMEK).
ConclusionOverall, DMEK proved superior over PK and DALK in terms of quality of vision, with PK offering slightly better outcomes than DALK in most visual function parameters under evaluation.
Se diseñó un estudio en un único centro y transversal para evaluar y comparar la calidad de la visión subjetiva de los pacientes intervenidos de queratoplastia penetrante (QP), queratoplastia lamelar anterior profunda (QLAP) y queratoplastia endotelial de membrana de Descemet (DMEK).
MétodosSe incluyó a cuarenta y seis pacientes previamente intervenidos de QP (22 ojos), QLAP (7 ojos) y DMEK (17 ojos). La evaluación visual incluyó la refracción esférica y cilíndrica, la agudeza visual de lejos corregida (AVDC), la sensibilidad al contraste fotópica (SC), la calidad óptica, medidas con el HD Analyzer (índice de dispersión objetiva [OSI], punto de corte MTF y ratio Strehl), así como la aberrometría ocular y corneal, medidas con el KR-1W Wavefront Analyzer.
ResultadosSe encontraron diferencias estadísticamente significativas entre los grupos en cuanto a edad (p=0,006, los pacientes de DMEK eran mayores) y el tiempo transcurrido desde la cirugía (p<0,001, tiempo superior para los pacientes de QP). No se encontraron diferencias estadísticamente significativas en cuanto a AVDC entre las técnicas. Se encontraron diferencias entre los grupos en cuanto a SC en 12 (p=0,007) y 18 (p<0,001) ciclos por grado, obteniendo DMEK y QLAP los mejores y peores resultados, respectivamente. Se encontraron diferencias en cuanto a calidad óptica entre las técnicas (OSI, p=0,004; punto de corte MTF, p=0,048; ratio Strehl p=0,022), reflejando DMEK los mejores resultados. Los mejores y peores valores en cuanto a aberraciones oculares y corneales fueron registrados por los pacientes de QLAP y DMEK, respectivamente. Se hallaron diferencias entre grupos en cuanto a astigmatismo corneal (p<0,001; -3,31±2 D en QP; -2,68±0,94 D en QLAP; -1,09±0,62 D en DMEK).
ConclusiónEn general, DMEK demostró ser superior a QP y QLAP en términos de calidad de visión, y QP ofreció mejores resultados que QLAP en la mayoría de los parámetros de la función visual evaluados.
Nowadays, many options are available to the corneal transplant surgeon for the treatment of corneal disorders. The keratoplasty surgical procedure has been modified to improve drawbacks associated with penetrating keratoplasty (PK), including delayed wound healing, major vulnerability to trauma, risk of immune rejection, unpredictable refractive outcomes, prolonged visual rehabilitation and high or irregular astigmatism.1,2 Although PK, in which the full corneal thickness is replaced, remains the gold standard,3 current keratoplasty procedures focus on replacing only the essential amount of tissue (also known as “selective keratoplasty”). Thus, in deep anterior lamellar keratoplasty (DALK),4 the whole corneal tissue is replaced with the exception of Descemet membrane and endothelium; in Descemet membrane endothelial keratoplasty (DMEK),5,6 the Descemet membrane and endothelium are replaced by the corresponding layers from the donor cornea; and in Descemet stripping (automated) endothelial keratoplasty (DSEK or DSAEK)7,8 the Descemet membrane and endothelium are replaced by a thin layer of donor stroma, Descemet membrane and endothelium. Lamellar corneal grafts have proved superior in terms of fast visual rehabilitation and more predictable refractive outcomes, requiring only partial rather than full-thickness incisions.9 Besides, DMEK has been reported to provide similar endothelial cell count but higher rebubbling rate than other endothelial keratoplasty techniques, while also restoring physiologic pachymetry.10,11
The present study aimed at describing and comparing visual outcomes of PK, DALK and DMEK. Previous researchers have assessed subjective and objective quality of vision of DALK with reference to PK. Thus, Güell and colleagues reported better best-corrected visual acuity (VA) and optical quality with PK than DALK, also noting a good correlation between these parameters.12 Ardjomand and co-workers also observed better spectacle-corrected VA in PK than DALK, with VA in DALK increasing in those eyes with lower (<20μm) thickness of the residual recipient stromal bed.13 These authors did not find any difference between PK and DALK in terms of contrast sensitivity (CS) and higher order aberrations (HOA). Pantanelli and colleagues reported better spectacle-corrected VA in PK than DALK, a difference that persisted even with full HOA correction through adaptive optics (HOA were worse in PK), although no differences in CS between PK and DALK were found.14 The same authors also evidenced the superiority of PK versus DSAEK in VA, but not in HOA, which they attributed to the longer time PK patients had for neural adaptation, and to the possible presence of corneal haze in DSAEK patients. Discrepancies amongst researchers persist, with reports describing similar best-corrected VA15,16 and HOA3,17 in PK and DALK, while others note a better performance of PK over DALK in both visual function parameters.18–20 Fewer studies have explored the visual outcome of DMEK, probably because this challenging technique is not yet widely spread. However, all these reports suggest that DMEK may be a superior technique in terms of fast visual recovery, less refractive changes, and best-corrected visual acuity when compared with DSAEK, as well as presenting with reduced posterior HOA than PK and DSAEK.10,21
Given the relatively small volume of published research addressing the objective and subjective quality of vision of patients following PK, DALK and DMEK, the purpose of the present single-center, cross-sectional study was to evaluate and compare the visual outcomes of these techniques in terms of visual acuity, contrast sensitivity, optical quality and higher-order aberrations. Although it may be argued that the decision of the corneal surgeon to select a particular technique is commonly governed by the characteristics of the condition (i.e., affecting the whole cornea or being limited to certain layers), in some instances this choice may be influenced by other factors such as expertise with a technique or expected visual outcomes. The findings of the present research may provide information to assist these decisions.
Material and methodsStudy sampleForty-six consecutive patients (23 females) who had previously undergone PK (22 eyes), DALK (7 eyes) or DMEK (17 eyes) surgery were included in the study. Twenty-two eyes were right eyes (48%) and 24 left eyes (52%). All patients attended the Cornea, Cataract and Refractive Surgery Unit, Instituto de Microcirugía Ocular (IMO), Barcelona, Spain, between January and June 2015 for follow-up visits of their procedures. Age of patients ranged between 23 and 78 years, with a mean age (±standard deviation) of 53.2 (±14.7) years. Exclusion criteria were concomitant ocular conditions known to influence visual outcome such as corneal opacities, uveitis, manifest cataracts, posterior capsular opacities, vitreous or retinal abnormalities and vitretomized eyes. Patients who had undergone post-keratoplasty corneal refractive surgery were also excluded, as were those unable to understand or comply with the instructions required for objective and subjective visual function assessment.
All patients received information regarding the procedures and associated possible complications and written informed consent was obtained. The study was conducted in accordance with the Declaration of Helsinki tenets of 1975 (as revised in Tokyo in 2004) and received the approval of an institutional ethical board (IMO).
Surgical proceduresAll corneal surgeries had been conducted by the same surgeon (JLG) at the Cornea and Refractive Surgery Unit, Instituto de Microcirugía Ocular (IMO), Barcelona, Spain. Surgeries were executed according to the previously described procedure for PK, DALK and DMEK.22–24 At the time of measurements all sutures inserted during the surgical intervention had been removed.
Visual function evaluationFollowing retinoscopy and subjective refraction, corrected distance high-contrast monocular visual acuity (DCVA) was measured in logMAR units with the Early Treatment Diabetic Retinopathy Study (ETDRS) charts (Optec 6500, Stereo Optical Co., Inc., Chicago, IL) at a viewing distance of 4m and under photopic conditions (85cd/m2). Contrast sensitivity (CS) was assessed with the CSV-1000 test (Vector Vision, Inc, Greenville, OH) placed at 2.5m. This test presents a translucent chart divided into four sine-wave grating stimuli at spatial frequencies of 3, 6, 12 and 18 cycles per degree (cpd) and eight levels of contrast. A two-alternative forced choice paradigm was implemented for CS measures. The background illumination of the translucent chart is provided by the fluorescent luminance source of the instrument, that is, it is independent of room illumination. Best distance correction was employed during all CS measurements.
Optical quality was assessed with the HD Analyzer (Visiometrics S.L., Spain). The HD Analyzer employs a double-pass system to evaluate the retinal image degradation of a point-source object.25 Double-pass images contain information about aberrations and scattering.26 Explored parameters were the objective scattering index (OSI), calculated as the ratio between the light reaching an annular area ranging from 2 to 20minute of arc from the central peak of maximum intensity and that of the central 1minute of arc,27 the modulation transfer function cut-off frequency (MTF cut-off), which is the spatial frequency corresponding to a 0.01 MTF value (the MTF value is calculated from the root square of the modulus of the Fourier transform of the double pass image), and the Strehl ratio, defined as the ratio under the measured MTF curve and the curve that would be obtained if the eye was free of aberrations.28 All measurements were performed with full spherical and cylindrical correction and for a 4mm pupil.
Finally, aberrometry data was obtained with the KR-1W Wavefront Analyzer (Topcon Medical Systems, Inc., Oakland, NJ). This instrument combines a Hartmann–Shack wavefront analyzer with a Placido disc-based anterior corneal topographer to provide ocular and anterior corneal aberrometry information, respectively (corneal aberrations are calculated from elevation data and subsequently transformed to wavefront Zernike polynomials). A pupil diameter configuration of 4mm was used to determine total ocular and anterior corneal HOA as the root mean square (RMS) values of all Zernike coefficients of order 3rd to 8th. The same instrument was employed as a topographer to obtain anterior corneal astigmatism, objective refraction, as well as to determine pupil diameter under mesopic conditions (5cd/m2). Internal aberrations were obtained by subtracting corneal aberrations from ocular aberrations.
All procedures were conducted by an experienced optometrist (CG), masked to the type of surgery being evaluated. Aberrometry and optical quality measurements were repeated three times and the average was used for statistical analysis.
Data analysisStatistical analysis was performed with the IBM SPSS software for Windows (IBM Corporation, Armonk, NY). All data were examined for normality with the Kolmogorov–Smirnov test, which revealed compliance with a normal distribution. Accordingly, descriptive statistics are summarized as mean±SD. An analysis of variance test (ANOVA) was employed to investigate the statistical significance of the differences between PK, DALK and DMEK for each variable under evaluation and, when differences reached statistical significance, the Tukey post hoc test was employed for pair-wise analysis, thus taking into consideration family-wise error-rate. A p-value of 0.05 or less was considered to denote statistical significance throughout the study.
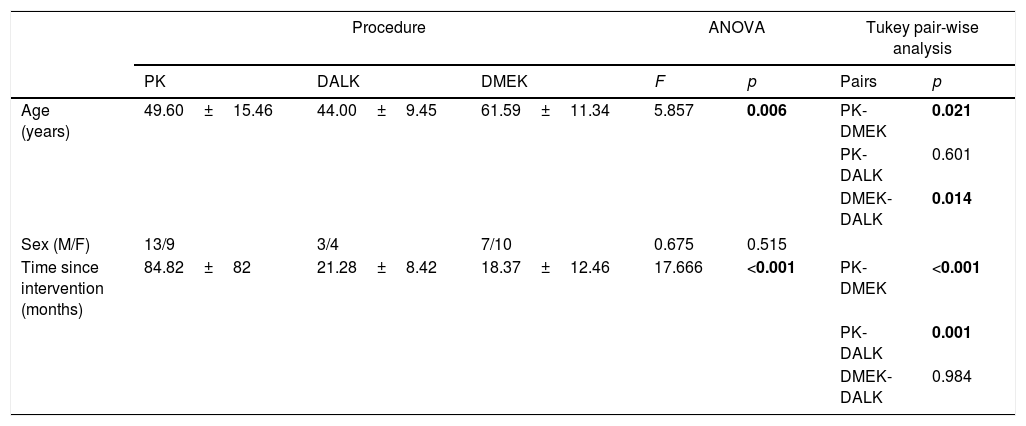
ResultsDemographic data for PK, DALK and DMEK groups is summarized in Table 1, which also shows time (in months) since surgery. An ANOVA analysis revealed statistically significant differences both in age (F=5.857; p=0.006) and time since surgery (F=17.666; p<0.001). When submitted to a Tukey post hoc test, pair-wise differences in age were found between DMEK and PK and between DMEK and DALK, with DMEK patients (61.59±11.34 years) being older than PK (49.60±15.46 years) and DALK patients (44.00±9.45 years). Differences were also found in time since surgery between PK and DALK and between PK and DMEK, with time since PK being much longer (84.82±52.21 months) than time since DALK (21.28±8.42 months) and time since DMEK (18.37±12.46 months). Main reasons for intervention were Fuchs endothelial dystrophy (15 patients) and keratoconus (15 patients).
Demographic details, presented as mean±standard deviation (SD), of PK, DALK and DMEK patients. Results of the ANOVA test and post hoc Tukey pair-wise analysis are shown. Any p-value<0.05 (in bold) denotes statistical significance.
| Procedure | ANOVA | Tukey pair-wise analysis | |||||
|---|---|---|---|---|---|---|---|
| PK | DALK | DMEK | F | p | Pairs | p | |
| Age (years) | 49.60±15.46 | 44.00±9.45 | 61.59±11.34 | 5.857 | 0.006 | PK-DMEK | 0.021 |
| PK-DALK | 0.601 | ||||||
| DMEK-DALK | 0.014 | ||||||
| Sex (M/F) | 13/9 | 3/4 | 7/10 | 0.675 | 0.515 | ||
| Time since intervention (months) | 84.82±82 | 21.28±8.42 | 18.37±12.46 | 17.666 | <0.001 | PK-DMEK | <0.001 |
| PK-DALK | 0.001 | ||||||
| DMEK-DALK | 0.984 | ||||||
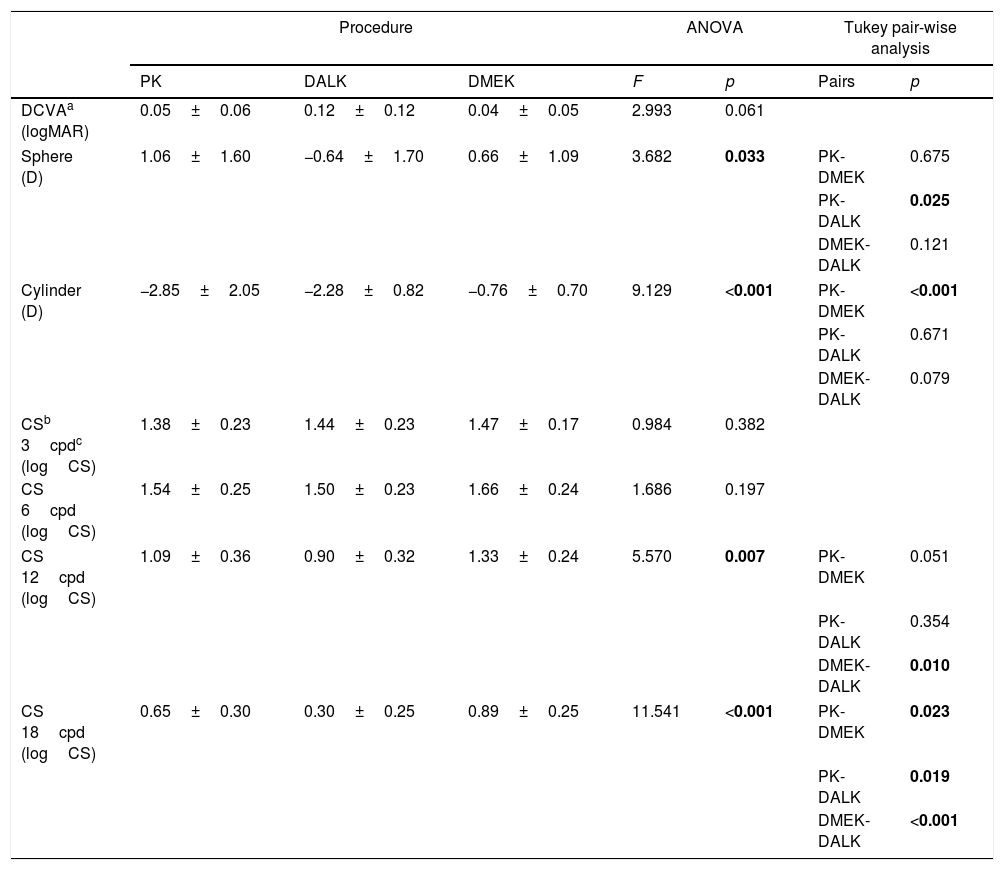
Refractive sphere and cylinder outcomes, as well as DCVA and CS for each group of patients, are shown in Table 2. Statistically significant between-group differences in both refractive sphere (F=3.682; p=0.033) and cylinder (F=9.129; p<0.001) were encountered which, when examined pair-wise, were found to originate in the differences between PK and DALK in spherical refraction and between PK and DMEK in cylinder. The largest and smallest refractive astigmatism corresponded to eyes intervened of PK (−2.85 D±2.05 D) and DMEK (−0.76 D±0.70 D), respectively. In terms of CS, statistically significant between-group differences were encountered at high spatial frequencies: 12cpd (F=5.570; p=0.007) and 18cpd (F=11.541; p<0.001). In particular, at 18cpd, all pair-wise analyses revealed significant differences, with DMEK (0.89±0.25) and DALK (0.30±0.25) patients achieving the best and worst CS outcomes, respectively. No statistically significant differences were found in DCVA.
Refractive and visual outcomes, presented as mean±standard deviation (SD), of PK, DALK and DMEK patients. Results of the ANOVA test and post hoc Tukey pair-wise analysis are shown. Any p-value<0.05 denotes statistical significance.
| Procedure | ANOVA | Tukey pair-wise analysis | |||||
|---|---|---|---|---|---|---|---|
| PK | DALK | DMEK | F | p | Pairs | p | |
| DCVAa (logMAR) | 0.05±0.06 | 0.12±0.12 | 0.04±0.05 | 2.993 | 0.061 | ||
| Sphere (D) | 1.06±1.60 | −0.64±1.70 | 0.66±1.09 | 3.682 | 0.033 | PK-DMEK | 0.675 |
| PK-DALK | 0.025 | ||||||
| DMEK-DALK | 0.121 | ||||||
| Cylinder (D) | −2.85±2.05 | −2.28±0.82 | −0.76±0.70 | 9.129 | <0.001 | PK-DMEK | <0.001 |
| PK-DALK | 0.671 | ||||||
| DMEK-DALK | 0.079 | ||||||
| CSb 3cpdc (logCS) | 1.38±0.23 | 1.44±0.23 | 1.47±0.17 | 0.984 | 0.382 | ||
| CS 6cpd (logCS) | 1.54±0.25 | 1.50±0.23 | 1.66±0.24 | 1.686 | 0.197 | ||
| CS 12cpd (logCS) | 1.09±0.36 | 0.90±0.32 | 1.33±0.24 | 5.570 | 0.007 | PK-DMEK | 0.051 |
| PK-DALK | 0.354 | ||||||
| DMEK-DALK | 0.010 | ||||||
| CS 18cpd (logCS) | 0.65±0.30 | 0.30±0.25 | 0.89±0.25 | 11.541 | <0.001 | PK-DMEK | 0.023 |
| PK-DALK | 0.019 | ||||||
| DMEK-DALK | <0.001 | ||||||
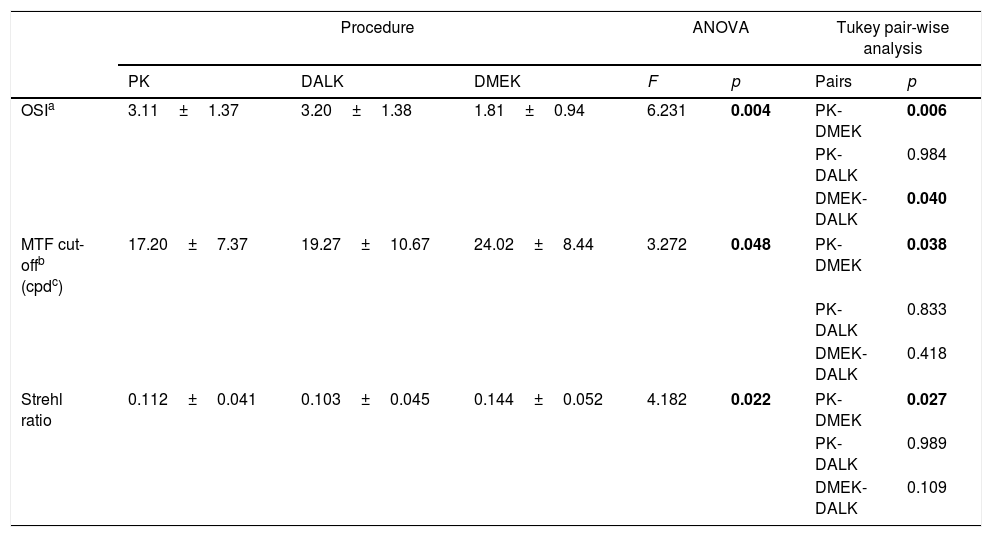
Table 3 displays a summary of the HDA measurements. An ANOVA test disclosed statistically significant differences in OSI (F=6.231; p=0.004), MTF cut-off (F=3.272; p=0.048) and Strehl Ratio (F=4.182; p=0.022) among the three procedures. A post hoc pair-wise analysis revealed statistically significant differences between PK and DMEK in all these parameters, as well as between DALK and DMEK in OSI. Overall, DMEK presented the best outcome in terms of optical quality and scattering, with PK performing slightly better than DALK.
Outcomes from the HD Analyzer, presented as mean±standard deviation (SD) of PK, DALK and DMEK patients. Results of the ANOVA test and post hoc Tukey pair-wise analysis are shown. Any p-value<0.05 denotes statistical significance.
| Procedure | ANOVA | Tukey pair-wise analysis | |||||
|---|---|---|---|---|---|---|---|
| PK | DALK | DMEK | F | p | Pairs | p | |
| OSIa | 3.11±1.37 | 3.20±1.38 | 1.81±0.94 | 6.231 | 0.004 | PK-DMEK | 0.006 |
| PK-DALK | 0.984 | ||||||
| DMEK-DALK | 0.040 | ||||||
| MTF cut-offb (cpdc) | 17.20±7.37 | 19.27±10.67 | 24.02±8.44 | 3.272 | 0.048 | PK-DMEK | 0.038 |
| PK-DALK | 0.833 | ||||||
| DMEK-DALK | 0.418 | ||||||
| Strehl ratio | 0.112±0.041 | 0.103±0.045 | 0.144±0.052 | 4.182 | 0.022 | PK-DMEK | 0.027 |
| PK-DALK | 0.989 | ||||||
| DMEK-DALK | 0.109 | ||||||
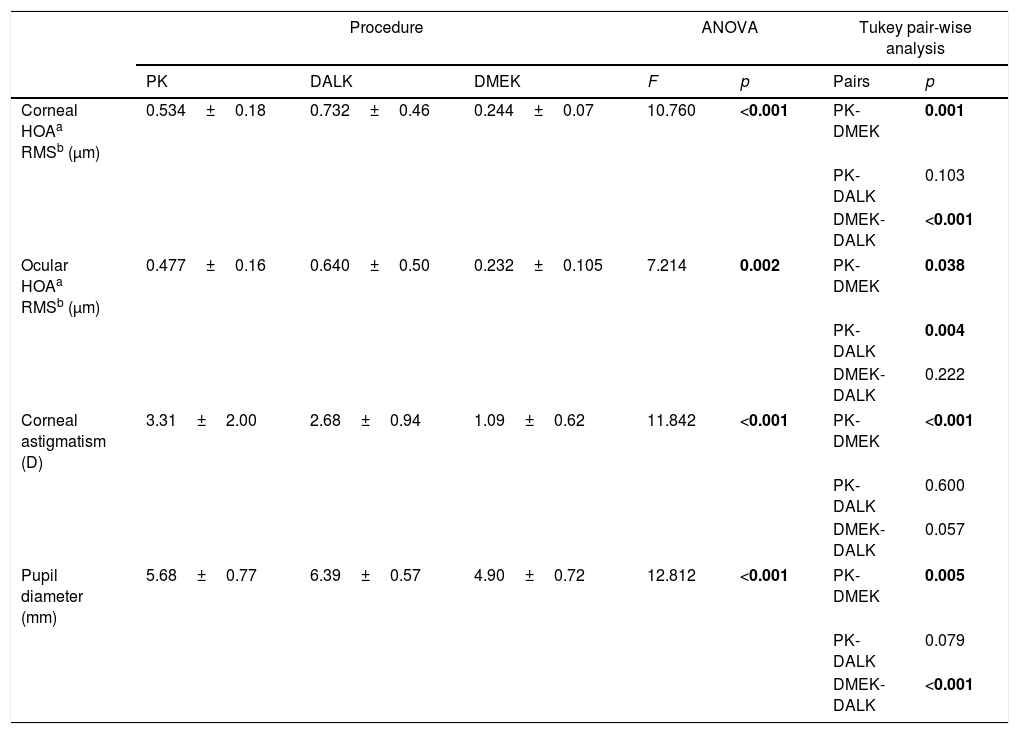
The measurements of the KR-1W are shown in Table 4. Statistically significant between-group differences were found in all parameters under evaluation. The highest and lowest ocular and corneal HOA values corresponded to DALK and DMEK, respectively, with statistically significant differences between PK and DMEK and between DALK and DMEK, and a similar performance of PK and DALK. Calculated mean internal HOAs were −0.57μm in PK, −0.92μm in DALK and −0.12μm in DMEK. Corneal astigmatism was also different between the three procedures (F=11.842; p<0.001), with statistically significant pair-wise differences between PK and DMEK and between DALK and DMEK. Corneal astigmatism was highest in PK patients (−3.31±2.00 D), followed by DALK patients (−2.68±0.94 D), and DMEK patients (−1.09±0.62 D). Finally, between-group differences in pupil diameter were found (F=12.812; p<0.001). Patients intervened with DALK had larger pupils than PK patients and DMEK patients, although statistically significant differences were only found between the pairs PK – DMEK and DMEK – DALK.
Results of the KR-1W Wavefront Analyzer, presented as mean±standard deviation (SD) of PK, DALK and DMEK patients. Results of the ANOVA test and post hoc Tukey pair-wise analysis are shown. Any p-value<0.05 denotes statistical significance.
| Procedure | ANOVA | Tukey pair-wise analysis | |||||
|---|---|---|---|---|---|---|---|
| PK | DALK | DMEK | F | p | Pairs | p | |
| Corneal HOAa RMSb (μm) | 0.534±0.18 | 0.732±0.46 | 0.244±0.07 | 10.760 | <0.001 | PK-DMEK | 0.001 |
| PK-DALK | 0.103 | ||||||
| DMEK-DALK | <0.001 | ||||||
| Ocular HOAa RMSb (μm) | 0.477±0.16 | 0.640±0.50 | 0.232±0.105 | 7.214 | 0.002 | PK-DMEK | 0.038 |
| PK-DALK | 0.004 | ||||||
| DMEK-DALK | 0.222 | ||||||
| Corneal astigmatism (D) | 3.31±2.00 | 2.68±0.94 | 1.09±0.62 | 11.842 | <0.001 | PK-DMEK | <0.001 |
| PK-DALK | 0.600 | ||||||
| DMEK-DALK | 0.057 | ||||||
| Pupil diameter (mm) | 5.68±0.77 | 6.39±0.57 | 4.90±0.72 | 12.812 | <0.001 | PK-DMEK | 0.005 |
| PK-DALK | 0.079 | ||||||
| DMEK-DALK | <0.001 | ||||||
Published literature is inconclusive regarding the superiority of a particular keratoplasty technique in regards to optical quality. Differences in study design, instrumentation and follow-up time, amongst other factors, may account for these discrepancies. In the present study, we aimed at examining and comparing objective and subjective visual quality in patients intervened with PK, DALK and DMEK. Although all procedures were conducted by the same experienced surgeon and in the same clinical setting, some study design limitations remained unresolved, mainly regarding between-group differences in age of patients and time since surgery. Indeed, whereas most DMEK patients continue to wear their own glasses after surgery, on account of the minor change in refraction associated with this technique, stability of visual acuity and refraction in PK may require a few months.29 During this time, PK patients may have time for neural adaptation to their post-operative aberrations.14 In summary, different results may have been obtained with a sample better matched in time since surgery.
Overall, patients intervened with DMEK were found to outperform PK and DALK patients in most of the examined visual function and refractive parameters, including refractive and corneal astigmatism, contrast sensitivity at high spatial frequencies, optical quality, scattering and corneal and ocular HOAs. It must be noted, however, that DMEK patients were older than PK and DALK patients, resulting in statistically significant differences in pupil diameter that may partially account for the superiority of this procedure in terms of CS. In contrast, albeit optical quality and aberrations are influenced by pupil diameter, all these measurements were conducted with an artificial pupil of 4mm, that is, pupil diameter may not be considered as a confounding variable for these parameters.
No statistically significant differences in DCVA were found between the techniques. These results are in agreement with previous reports comparing PK and endothelial keratoplasty procedures,30,31 as well as PK and DALK,15,16 although other authors describe a better performance of PK over DALK in DCVA.18–20 It is interesting to note that many of these authors report that, in general, patients intervened with any type of keratoplasty fail to reach their full visual potential. In this regards, 7 out of 22 PK, 3 out of 7 DALK and 3 out of 17 DMEK patients had DCVA worse than 0.1logMAR (0.8 decimal) at the time of the follow-up appointment. Increased scattering and HOA may account for the inability of some of these patients to overcome a particular visual acuity threshold. However, the encountered between-group differences in HOA and optical quality were not accompanied by corresponding differences in DCVA. This finding may suggest that either different mechanisms may be governing the relationship between these parameters in PK, DALK and DMEK or that DCVA is not as sensitive as CS at high spatial frequencies, in which DMEK patients scored better results than PK and DALK patients, to compare visual quality between keratoplasty techniques. It may be worth noting that CS at middle and high spatial frequencies has been documented to be particularly useful for target detection and identification tasks, even in patients in whom visual acuity is not excellent.32
Regarding the superiority of DMEK in terms of both ocular and corneal HOAs, it must be noted that the Placido disk/Hartmann–Shack configuration of the KR-1W allows for the measurement of ocular, that is, wavefront, aberrations, and of anterior corneal aberrations, which are determined from topographical height data. Internal corneal aberrations, including those originating at the posterior cornea and at the lens, may be estimated by subtracting anterior corneal from ocular HOAs. Thus, given mean internal HOAs of −0.57μm in PK, −0.92μm in DALK and −0.12μm in DMEK, the actual impact of posterior HOAs on visual quality in DMEK patients was probably not significant.33,34 These results, which are in agreement with previous reports,21 are not unexpected, as the change in refractive index between the posterior cornea and the aqueous humor is smaller than the change occurring at the anterior surface between air and the cornea/tear film. Further research, including the evaluation of posterior height data, is needed to better understand this finding, however. Overall, DMEK, as the less invasive procedure of the three, was also found to present the best outcome in terms of optical quality and scattering.
Finally, it may be worth mentioning that between-group differences in age (DMEK patients were older) and particularly in time since surgery (more time in PK) may have resulted in an underestimation of the differences between the techniques. In effect, the loss with age of the ability of the posterior cornea to compensate anterior corneal HOA has been previously described,35 as has the positive effect of neural adaptation on visual quality, particularly in PK patients.14 In addition, given the recruitment difficulties encountered with DALK patients, with only 7 subjects in this group, the possibility of Type II error may not be ruled out, i.e., it may be speculated whether with a larger, more balanced sample, other statistically significant differences between techniques may have been uncovered.
In conclusion, as far as we know the present study is one of the first reports comparing quality of vision in PK, DALK and DMEK patients, and one of the few exploring ocular wavefront, as well as, anterior corneal height-data based aberrations.36 Although some study limitations remain that warrant further investigation, our findings give support to the overall superiority of DMEK over PK and DALK. The lack of statistically significant differences in DCVA between the procedures highlights the advantages of exploring other visual function parameters, such as CS, optical quality, scattering and HOAs, to assess the subtle differences in visual quality of these patients. Finally, in view of the present findings, we would advise eye care providers to manage these patients with contact lenses, instead of glasses, to improve post-operative VA, contrast sensitivity and to reduce HOA.
Conflicts of interestThe authors have no conflicts of interest to declare.





