






The aim of the study was to verify the hypotheses that vergence-accommodation conflict (VAC) induced with head-mounted device (HMD) could cause symptoms in relation to changes in the accommodative-vergence system. In order to test this hypothesis, the Virtual Reality (VR) exposures were carried out in two types of VAC: VACsmall and VAClarge.
MethodEighteen females, with a mean age of 22.5 ± 2.0 years, participated in two 30-minutes sessions with VR, which were separated by at least one week. Two sessions were differentiated by intensity of VAC presented in the VR system (VACsmall and VAClarge). Visual parameters were measured such as associated and dissociated phoria, accommodative response, the near point of convergence (NPC), fusional vergence ranges (FVR) and subjective complaints were measured using Simulator Sickness Questionnaire (SSQ). The parameters were measured immediately before (Pre-test) and after (Post-test) the VR exposure.
ResultsThe subjective symptoms as nausea, oculomotor disorders and disorientation increased significantly after 30-minutes of exposure on VAClarge (P<0.05). The associated and dissociated phoria, lag of accommodation, FVR and the NPC did not significantly change after the VR exposure (P>0.05).
ConclusionShort-term use of HMD (30-min) did not significantly affect accommodative-vergence functions regardless of the size of VAC (VACsmall and VAClarge). However, the level of symptoms increased after VR sessions, which was probably related to inappropriate oculo-vestibular relationship.
In recent years, the usefulness of VR has increased due to technological development. As a result, many researchers are trying to answer whether time spent in VR could affect vision. Creating a three-dimensional (3D) space in close proximity to the eyes remains a key element for designers. When designing such an image, any conflict between accommodation (the response of the crystalline lens) and vergence (the alignment of the eyes), can lead to visual complaints called asthenopia. Asthenopic symptoms, such as periodic blurred vision, eye fatigue and burning, a feeling of sand under the eyelids, headaches and eye pain, loss of concentration, or even periodic diplopia, often occur in people with vergence disorders1-6 or dyslexia.6-9 The mismatch between the accommodative and vergence stimuli that occurs when using a HMD may therefore be the cause of the asthenopic symptoms that VR users often report after prolonged use.
VR is a computer-simulated artificial multi-sensory (visual, auditory, even tactile stimuli) 3D environment that can imitate the properties and images of the physical world. It can also be entirely imaginary, or a combination of both.10 When looking for differences between the real world and the virtual world, it should be noted that in VR, regardless of whether the gaze is focused on something in the far or in the near distance, all objects will remain sharply visible for the viewer11. Thus, the brain has to decide which image is important at a given moment and which should be neglected. To achieve clear vision in 3D space, the eyes must adjust the power of the crystalline lens to the distance of the observed objects (accommodation process). In addition, the visual axes of both eyes must be properly aligned (vergence process).12 It creates images on the retinas of both eyes that are fused in the visual cortex to form a single, clear, binocular image of the observed scene. The accommodation and vergence systems are neurally coupled, and their interaction is essential for proper binocular vision and depth perception.13 Accommodative response is accompanied by simultaneous change in the ciliary muscle tension and a change in the power of the crystalline lens (accommodation response).12 When the outputs of two systems don't match, and the difference goes beyond the specified depth of the Panuma area, it creates a conflict between vergence and accommodation, known as VAC. VAC is described as the difference between the required vergence response and ocular accommodation and vice versa.
In HMD, the level of the accommodative stimulus is constant due to the fact that the image being viewed is placed at a fixed distance, but there are different vergence stimuli for the right eye and for the left eye,14 resulting in VAC. If VAC is large, asthenopic symptoms may occur.15
Studies indicate that VR may cause other visual symptoms such as eye-strain, vertigo, dizziness, disorientation or headache may appear already after 11–20 min of playing games.16-17 What's more, the longer the time is, the bigger complaints users might have to deal with.18 The situations described above lead one to search for the causes of the symptoms associated with the use of HMD. So far, it has not been explained what causes such complaints, whether they are visual in nature or due to a mismatch between visual and vestibular information. Someone might suggest that one of the main causes of the symptoms is the VAC present in the HMD technology discussed above.
The study was aimed to verify if VAC induced with HMD can cause symptoms of asthenopia in relation to changes in the accommodative-vergence system. In order to test this hypothesis, the VR exposures were carried out in two types of VAC: small and large. If visual symptoms were related to VAC, we would expect the symptoms to depend on the size of the conflict as well as on changes in the vergence-accommodation system.
Materials and methodsSubjectsThe participants were recruited from the student population of Adam Mickiewicz University in Poznan, attracted by additional points to their modules grades.
Inclusion criteria were: age between 18 and 30; best corrected visual acuity (Vis => 0,8), binocular vision in normal range (stereopsis better than 100′’), amplitude and facility of the accommodation in normal range to age, no history of strabismus or any neurological disease or injury.
Exclusion criteria were: amblyopia or any eye disease, strabismus, impaired binocular vision (suppression or double vision, lack of stereovision or stereopsis lower than 100′’), any neurological disease, epilepsy, vertigo or dizziness, neurological injury. Medical history information was obtained, moreover visual acuity, ocular alignment and binocular vision were assessed by classic optometric methods, including Snellen visual acuity testing, dynamic retinoscopy, prismatic cover test, Worth 4-dot testing and Titmus stereo vision test, following the procedures described in Grosvenor Optometry.19
After applying the criteria, 26 people (23 women and 3 men) were qualified, however, 8 people did not show up for the second session. Finally, 18 subjects were included in the statistical analyses. They were women aged from 19 to 27 years old (average age was 22,5). The visual parameters of each person were within normal limits for age, and the refractive error, if present, were corrected with glasses or contact lenses.
Apparatus and proceduresThe main experiment consisted of 3 parts. Part1: Pre-test, Part2: playing VR game, Part3: Post-test (Fig. 1).
Pre- and Post-tests
Procedures were performed in the same order. Firstly, the Simulator Sickness Questionnaire (SSQ) was carried out to evaluate the level of visual and vestibular symptoms caused by virtual reality systems. In this survey, the subjects assessed the intensity of the 18 symptoms on a scale from 0 (no complaints) to 3 (significant complaints) before and after exposure to a factor causing it. The complaints were grouped into three non-mutually exclusive categories: nausea, oculomotor disorders and disorientation as suggested by Bimberg et al.20
Secondly, accommodative response was tested by the Speedy method, using a Righton Speedy-K autorefractometer (autorefractometer, SN:3,300,199, Japan). Using this device it is possible to access the lag of accommodation by comparing refractive state of the eye with required response of accommodation when stimulus for accommodation changes.21-22 The accommodative response was measured from stimulus zero to 3 D, with changes in 0.5 D increments.23 Next the lag of accommodation was calculated as a difference between required and executed response of accommodation. Positive linear function (y=ax+b) was fitted to the values of individual lags of accommodation, which gave the coefficient a which reflected the slope of the function. The higher the value of coefficient a, the greater was the increase of lag.
The measurements of associated phoria were taken using the Hoya EyeGenius system. The system consists of three elements: an iPad that controls both the distance display and the near display: the distance screen (at 4 metres) and the near screen (40 cm). In the case of distance fixation disparity measurement, it is necessary to use polarizing glasses, and when using the near device, the subjects removed the glasses due to the fact that the near panel has high-quality polarization.21
The rest of the procedures used for visual function assessment are used in standard optometric offices.12,19,23 The measurements of dissociated heterophoria at distance was evaluated with Maddox stick method using phoropter with Maddox rod and Risley prisms. Near phoria was measured with Maddox stick but to control accommodation letter plates was used (modified Thorington method).
Fusional vergence ranges were measured and far (4 m) and near (40 cm) distance with van Graffe method using Risley prisms with a phoropter. The last measurement was near point of convergence (NPC) which is the point of the intersection of the lines of sight of the eyes when maximum convergence is utilized. NPC was measured with push-up method using pencil and of ruler. Break of fusion was reported when one eye lose fixation or participant reported diplopia and recovery of fusion was noted when the participant notice single vision again.24
Playing VR gameDuring 30 min, participants played a game Underwater Treasures (Fig. 2) using the HMD (Remmed, Gogle Pico Neo 1, Poland). Visual stimuli from both eyes were seen simultaneously to induce fusion. The main goal for the participants was to locate the stimulus, which was yellow diamonds on the arms of individual starfish and shoot them with pink bullets. The more points the subject scored, the faster the starfish moved, However the size of the diamond stimulus remained the same.

In HMD, conflict might be manipulated by displaying the image for the right and left eyes independently, with slightly different elements. That's why the brain is able to create a projection of virtual space. In HMD, the stimulus for accommodation remains constant (at 1.5 meter), while the stimulus for vergence can be manipulated.25 In the VACsmall condition (block 1) the vergence stimulus was similar to an accommodation stimulus. Contrary, in the VAClarge (block 2) condition the vergence stimulus was significantly separated from the accommodation stimulus. The block 1 and 2 were carried out in counterbalanced order, with at least one week off between studies.
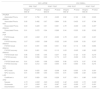
Statistical analysesStatistical analysis was carried out using the Statistica 13.1 software by Statsoft. In order to check whether the determined data had a normal distribution, the Shapiro-Wilk test (Table 1) was used. If the data met the condition of normality (P≥0.05). Since majority of the conditions had normal data distribution and many factors were examined, analyses of variance (ANOVA) with repeated measurements, was used for statistical analyses. Two factors were used for LAG of accommodation and slope of accommodative response function (parameter a): conflict (2 levels: VAClarge and VACsmall,), test (2 levels: Pre-test and Post-test). Three factors were investigated for phoria data: conflict (2 levels: VAClarge and VACsmall,), test (2 levels: Pre-test and Post-test), distance (2 levels: far and near). Also, three factors were used for NPC: conflict (2 levels: VAClarge and VACsmall,), test (2 levels: Pre-test and Post-test), fusion (2 levels: break and recovery). Four factors were investigated in vergence ranges data: conflict (2 levels: VAClarge and VACsmall,), test (2 levels: Pre-test and Post-test), prism base (2 levels: base in- and base-out) and fusion (2 levels: break and recovery).
Value for Shapiro-Wilk test and P-value for each parameter, BI- base in, BO- base out, FVR- fusional vergence ranges, NPC- near point of convergence, LAG- lag of accommodation, SSQ- simulator sickness questionnaire.
Parameters for non-normally distributed data have been presented in italics.
Non parametric test (Wilcoxon Match Pairs Test) was used to evaluate SSQ points since majority of parameters had data distribution far from normal.
Statistical significance was achieved, if P-value was < 0.05.
ResultsSimulator sickness questionnaireThe results of the SSQ are presented in Table 2. In the Post-test for both conflicts SSQ values exceeded the threshold of 20 points which is treated as critical. Comparing the median results of the SSQ, subjects reached more points in the Post-test than in the Pre-Test and it was true in both conflict conditions (VAClarge: Z = 3.00; P=0.003; VACsmall: Z = 2.07; P=0.038). In VAClarge the increase of symptoms was noted in the nausea (Z = 2.55; P=0.11), such as general discomfort, increased salivation, sweating, nausea, concentration problems, abdominal pain. It also affected disorientation components such as headache, blurred vision, dizziness with eyes open and closed (Z = 3.11; P=0.002) and oculomotor disorder (Z = 2.07; P=0.038).
The impact of VAC on individual categories of SSQ complaints survey, P25–25th percentile, P75–75th percentile, IQR-Interquartile range.
Furthermore, VACsmall also affected disorientation symptoms (Z = 2.10; P=0.036) but changes in the oculomotor disorder were close to significance (Z = 1.95; P=0.051).
Response of accommodationThe mean lag of accommodation in the Speedy method was similar for both conflicts (0.93 D for VACsmall and 0.97 D for VAClarge, F(1,16)=0.70, P=0.414; Fig. 3). No significant change in lag of accommodation between Pre- and Post-tests was found when both conflicts (VAClarge and VACsmall) were analysed separately, which was confirmed by the insignificant conflict x test interaction (F(1,16)=0.58, P=0.459).

Investigating the value of lag of accommodation in the Speedy method with increasing stimulus for accommodation, it was found that slope of accommodative function was similar in both conflict conditions. In the VACsmall the slope of the accommodative response (coefficient a) changed from 0.27 to 0.21 in Pre- and Post-test. In the VAClarge, the value of a-parameter was 0.24 in the Pre- and Post-test (F(1,16)=0.02, P=0.884; Fig. 4). There was no statistical difference in the value of the slope coefficient a.
Associated and dissociated phoria and near point of convergence in the pre- and post-test. Bars mean the standard error of mean.")
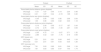
Some differences in the associated phoria at distance and at near were noticed after the exposure of the VAC, which was shown in Table 3. Significant test and conflict interaction (F(1,17)=5.43; P=0.032) suggested that in the VAClarge, the value of the associated phoria shifted in a positive direction from Pre- to Post-test but this shift was opposite in the VACsmall. However posthoc test did not prove these differences (P>0.05 for all comparisons). Associated phoria was also independent on the distance, which was proved by insignificant interaction between test, conflict and distance (F(1,17)=0.82, P=0.378).
The impact of the condition of vergence-accommodation conflict on the value of the associated and dissociated phoria, near point of convergence (NPC) in the pre-test and post-test, SD- standard deviation, SE- standard error, VAClarge - large vergence-accommodation conflict, VACsmall - small vergence-accommodation conflict.
The results of the dissociated heterophoria were also presented in Table 3. The mean value of this parameter measured at near distance was significantly higher than at far distance (mean effect of distance: F(1,17)=7.60, P=.013). The difference between heterophoria measured at different distances was comparable in both VACs, which was confirmed by insignificant interaction between conflict and distance (F(1,17)=0.83, P=0.375). Session with HMD did not significantly change the heterophoria in any of the studied conflicts (VAClarge and VACsmall), which was proved by the statistically insignificant relationship between conflict and test (F(1,17)=1.32, P=0.266), between test and distance (F(1,17)=1.08; P=0.314), as well as between conflict, test and distance (F(1,17)=3.09, P=0.097).
The results of NPC were presented in Table 3. No significant difference in the fusional break and recovery of NPC was observed between Pre- and Post-test (main effect of test: F(1,17)=1.80; P=0.197; test x fusion interaction: F(1,17)=0.12; P=0.736). Similarly, there was no effect of the conflict condition on the measured values of the NPC both at break of fusion and at the fusion recovery (interaction between conflict x test x fusion: F(1,17)=3.09; P=0.097).
Fusional vergence rangesTable 4. presents the mean values of distance FVR (dFVR) for both studied conflicts. Consistent with assumptions, the mean dFVR values for base-out prism (BO) were significantly higher than for base-in prisms (BI) (main effect of prism base: F(1,17)=18.10, P=0.001). As expected, the mean value for break of fusion was also higher than for recovery of fusion (main effect of fusion: F(1,17)=231.62, P<0.001). The average dFVR values were comparable in the Pre- and Post-tests (main effect of the test: F(1,17)=0.08, P=0.786). Likewise before, there was no impact of VR exposure on the mean values of dFVR in the Pre- and Post-tests when analyzing the BI and BO values separately (test x base interaction: F(1,17)=0.08, P=0.778), as well as when analyzing the parameters of breaking and recovery of fusion separately (test x fusion interaction: F(1,17)=0.15, P=0.700). What's more, the dFVR values did not change in the Post-test in relation to the Pre-test in any of the tested conflict conditions, what was confirmed by insignificant interactions between conflict, prism base, fusion and test (F(1,17)=0.56 P=0.464).
Mean values of near and distance Fusional Vergence Ranges [Δ] in the conditions VAClarge and VACsmall, SD- standard deviation, SE- standard error, dFVR- fusional vergence ranges at far distance, nFVR- fusional vergence ranges at near, VAClarge - large vergence-accommodation conflict, VACsmall - small vergence-accommodation conflict.
Values of the near fusional vergence range (nFVR) were presented in Table 4. In line with expectations, the mean values for break of fusion was also higher than for recovery of fusion (main effect of fusion: F(1,17)=61.10, P<0.001). The mean value of nFVR in the Post-test was comparable to the Pre-test (F(1,17)=0.44, P=0.514). Practicing with HMD also did not affect the nFVR values when measuring in the direction of base-in, and in the direction of base-out (test x base interaction: F(1,17)=1.04, P=0.323), as well as when break and recovery skills were tested (test x fusion interaction: F(1,17)=0.21, P=0.650). Similarly to dFVR, the use of HMD hadn't any influence on vergence ranges independent on conflict used (conflict x test interaction: F(1,17)=3.77, P=0.069), as well as when examining measurement of BO and BI prisms separately (conflict x test x base interaction: F(1,17)=0.64, P=0.434). Data remained statistically insignificant also when testing interaction between conflict, base, fusion and test (F(1,17)=1.75, P=0.203). Furthermore, the mean values of nFVR in both conditions (VAClarge and VACsmall) and in the Post- and Pre-tests were comparable, which was confirmed by the statistically insignificant interaction between the conflict and the test interaction (F(1,17)= 3.77, P=0.069), between conflict, test, and base interaction (F(1,17)=0.64, P=0.434), and between conflict, base, fusion, and test interaction (F(1,17)=1.75, P=0.203).
DiscussionThe aim of the study was to investigate whether VAC during 30 min of VR game play could affect visual functions such as binocular vision (associate and dissociated phoria or fusional vergence ranges), accommodative response and near point of convergence. Furthermore, it was investigated whether short-term exposure to VR games could increase the symptoms associated with nausea, oculomotor disorders and disorientation. The experiment was designed to test the hypothesis that asthenopic symptoms may be related to VAC induced by the HMD. For this purpose, the VR games were played in VAClarge and VACsmall conditions.
Studies focused on the changes in the tonic position of the eyes after prolonged work at near distances show that the change in heterophoria found after long convergence of the eyes induced by prisms (prismatic adaptation effect5) occurs in the tonic tensions of the oculomotor muscles system but not in the accommodative-vergence system,26 which results in eso-position of the eyes.27 Changes in tonic muscle tension are necessary to eliminate the vergence effort that occurs as a result of looking at one distance for a long time. Therefore, an adaptive process allows for maintaining visual comfort during prolonged visual work. Since no changes in the position of the phoria were reported in our study, there was no need for changes in the tonic tone of the oculomotor muscles. The obtained results in dissociated phoria showed that after 30-min of playing VR games in conditions of VAClarge, the eyes tended to converge (move toward eso-direction). Conversely, while exposed to VACsmall, an opposite effect was found (the position of the eyes was shifted in exo-direction), however this difference was not statistically significant. These findings align with other studies where HMD were used.28
VR games had no significant influence on the eyes’ position measured by phoria parameters. Again, there was no correlation between the value of VAC and phoria change. However, there was a certain tendency to change the dissociated phoria for a large conflict towards eso-shift, as well as towards exo-shift for a VACsmall. These changes remained statistically insignificant, but one could argue that using VR for a longer time, could change eyes position and interrupt in binocular position. In normal physiological conditions, any impairment in eye position (phoria differing from zero), is compensated by the vergence system, leading to proper binocular vision without any symptoms.
The results obtained in the current study showed no significant changes in fusional vergence ranges at far and at near distances, what was different in the study of Alhassan et al.29 They found changes in positive fusional convergence and negative fusional convergence at near, after 45 min of playing VR games. It is possible that using VR for up to 30 min, does not significantly affect the vergence system, but after a longer period, as in the study by Alhassan et al.,29 the parameters of vergence ranges are already altered.
In the current study, the VAC was generated by separating the stimuli for vergence (retinal images from both eyes) in front of the right and left eyes, but the stimulus for accommodation was stable for the whole VR game time. Working in those conditions for many minutes could induce changes in the accommodative response of the eyes. However, the obtained results showed that the accommodative response was not changed after the 30-minutes of playing VR games. In a similar study, Alhasan et al.29 observed no significant change in the lag of accommodation after a 45 min- session of VR games.
In the case of NPC, the changes in fusion break and fusion recovery were not statistically significant and should not affect the accommodative-vergence system or asthenopic symptoms. In the Yoon et al.’s study,30 the NPC significantly worsened after 2 h of using VR-HMD. The break and recovery point moved away on average by 2.75 cm, after a 2 hour session. Similar observations were described in the article by Kozulin et al.,31 where the break and recovery NPC was noticed to move away by 1 cm after 30-minutes of playing VR games and by 1.5 cm after 80-minute of playing VR games. However, these changes were not statistically significant and should not influence the symptoms. The obtained results confirmed that using the HMD for up to 30 min does not significantly affect changes in convergence skills.
The subjective symptoms were tested using the SSQ. As expected, the values for nausea, disorientation and oculomotor disorder in the Post-test were higher than in the Pre-test. When comparing the VAC conditions, it should be noted that the reported complaints were always greater in the conditions of VAClarge than in VACsmall condition. There were significant changes in all categories for VAClarge and in disorientation for VACsmall condition but oculomotor disorder was close to significance. We can assume that the increase in the symptoms was not induced by changes in the accommodative-vergence system since these parameters were not changed. The noticed symptoms were probably caused by the changes in the vestibular system. When using HMD, the changes in the retinal image are very dynamic, but do not coincide with the weak stimulation of the vestibular system. The lack of mutually appropriate stimulation between the visual and vestibular systems can cause sensations such as disorientation and nausea.
Taken together, the results from the current study suggest that the accommodation-vergence conflict does not have a significant impact on the accommodation-vergence system if the HMD is used no longer than 30 min. Short VR exposure seems to be safe for the visual system, without causing significant changes in visual functions. However, it is necessary to examine the influence of the session longer than 30 min on the visual parameters, and how people with binocular vision disorders will react to using HMDs. Such research was carried out by Yoon et al.30 on a similar group and statistically significant changes were observed in such parameters, as the near point of accommodation, both on the dominant eye and on the non-dominant eye.
Since symptoms such as disorientation, nausea and oculomotor disorder occurred in our study in VAClarge as soon as 30 min of VR exposure, but without changes in the oculo-visual parameters, this suggests that these symptoms are due to changes in the vestibular system. However, longer sessions may also cause changes in visual parameters and purely visual symptoms, indicating that working longer than 30 min may be very inconvenient for a user. It is therefore advisable to take breaks every 30 min when using the HMD to allow the visual system to recalibrate, minimizing the risk of changes to the visual system.
Limitation of the studyThis study is not without its limitations. Firstly, it's worth to note that the sample size comprised 18 subjects, all of whom were female and none of them struggled with binocular vision disorders. In future studies, it would be advisable to see if men and women respond to VR in the same way. In addition, it would be worthwhile to see how VR affects the visual system in people with binocular vision deficits. It is possible that VR games will be a significant strain on the visual system, but it is also possible that such sessions will be a form of exercise and improve specific visual functions. This question requires further research. Another limitation of the study was the short session time. We have shown that a 30-minute session does not significantly affect changes in functional visual parameters, but the situation would probably be much worse in a longer session. In future studies, it is advisable to extend the session and see after how many minutes significant functional changes appear. Given the potential influence of prolonged exposure, future investigations may benefit from gathering a larger sample size and extended VR exposure duration.
ConclusionsThe accommodative-vergence conflict generated by the 30-minutes of playing VR games did not significantly affect parameters of vergence and accommodation, independent of the VAC size. VAClarge increased the symptoms from all three groups: nausea, disorientation and oculomotor disorder, but VACsmall induced worsening in disorientation complains. The results suggest that changes in the functioning of the visual system itself are not responsible for the symptoms experienced after a short HMD session, but are most likely caused by a mismatch between visual and vestibular information.
AbbreviationsBI, base in; BO, base out; dFVR, fusional vergence ranges at distance; FVR, fusional vergence ranges; HMD, Head mounted device; nFVR, fusional vergence ranges at near; NPC, near point of convergence; Post-test, parameters measured immediately after VR gaming; Pre-test, parameters measured immediately before VR gaming; SSQ, Simulator Sickness Questionnaire; VAC, vergence-accommodation conflict; VAClarge, large vergence-accommodation conflict; VACsmall, small vergence-accommodation conflict; VR, virtual reality.
The authors declare that there is no conflict of interest or any financial disclosure that could interfere with the results of this study. The research was conducted using non-invasive optometric procedures, yet it was approved by the Adam Mickiewicz University Ethics Committee for matters concerning scientific research conducted with human participants: 16/2020/2021.





