



To determine the common symptoms in current soft contact lens (CL) wearers and their association with other factors among Nepalese population.
MethodsAll the current CL wearers who started to wear soft CL in Nepal Eye Hospital between July 2007 and June 2012 were invited for the participation. Frequency of the ten most common symptoms, divided into never, occasionally, frequently and consistent were recorded. Association between degree of symptoms with other factors, e.g. age, gender, profession, cigarette smoking, ethnicity, level of education and duration and wearing modality of CL wear were analyzed.
ResultsOut of 129 subjects participated in this study, 67% were female; the mean age of the subjects was 23.9±4.3 years. Ninety seven percent of them had at least one symptom occasionally or frequently or consistently. Discomfort was found in 88.4% of the total subjects. Other common symptoms were foreign body sensation in 73.6%, redness in 65.9%, reduced wearing time in 63.6% and dryness in 62.8%. Symptoms were found occasionally in the majority of subjects. Degree of symptoms was not associated with age, gender, profession, education status, ethnicity of subjects and duration or modality of lens wear (p>0.05) but was positively associated with passive cigarette smoking (p<0.001).
ConclusionAlmost all of the Nepalese soft CL wearers had some types of symptoms at least occasionally. Discomfort was the most common symptom. Degree of symptoms was associated with the passive smoking but not with other factors like age, sex, profession and duration of lens wear.
Determinar los síntomas comunes en los usuarios actuales de lentes de contacto blandas (LC), así como su asociación a otros factores, entre la población nepalí.
MétodosSe solicitó la participación de los usuarios actuales de LC, que habían comenzado a utilizar dichas lentes en el Hospital Ocular de Nepal entre julio de 2007 y junio de 2012. Se registró la frecuencia de los diez síntomas más comunes, divididos entre: nunca, ocasionalmente, frecuentemente y consistentemente. También se analizó la asociación entre el grado de los síntomas y otros factores tales como edad, sexo, profesión, consumo de cigarrillos, etnia, nivel de educación, duración y modalidad de uso de LC.
ResultadosDe los 129 sujetos participantes en este estudio, el 67% eran mujeres; la edad media de los sujetos fue de 23,9±4,3 años. El noventa y siete por ciento de ellos tenía al menos un síntoma de manera ocasional, frecuente, o consistente. El 88,4% de los sujetos reflejó malestar. Otros síntomas comunes fueron la sensación de cuerpo extraño en el 73,6% de los casos, el enrojecimiento en el 65,9%, la reducción del tiempo de uso en el 63,6%, y la sequedad en el 62,8%. Los síntomas fueron ocasionales en la mayoría de los sujetos. El grado de los síntomas no estuvo asociado a la edad, sexo, profesión, situación educativa, casta de los sujetos y duración o modalidad de uso de las lentes (p>0,05), aunque se asoció de modo positivo a la exposición pasiva al humo del trabaco (p<0,001).
ConclusiónCasi todos los usuarios nepalís de LC blandas reflejaron algún tipo de síntoma, al menos ocasionalmente. El malestar fue el síntoma más común. El grado de los síntomas se asoció a la exposición pasiva al humo de tabaco, pero no a otros factores tales como edad, sexo, profesión y duración del uso de las lentes.
Contact lens (CL) is one of the biomedical devices primarily used for refractive error correction. CL wearers may have significantly better quality of life in comparison to that of spectacle wearers.1 There are estimated 140 million people in the world wearing CL for the refractive purpose.2 And this number is increasing every year3 including in Nepal.4
Many of the soft CL wearers encounter clinically significant signs and/or symptoms with their lenses.5,6 Ocular symptoms may depend upon the ocular surface health of the CL wearers, lens design, materials and environmental factors. Symptoms associated with CL were found to increase throughout the day in some type of lenses.7 Ocular symptoms are the main causes of CL dissatisfaction and discontinuation.8 The primary reasons of CL discontinuation were found to be discomfort, dryness and red eyes.9 Refitting with new-generation of silicone hydrogel lenses can alleviate some of the common symptoms.5 In Nepal the majority of the CL wearers use conventional lenses.4,10 Moreover the pollution in city areas, where the majority of CL wearers live, is high.11 Therefore, higher rate of ocular symptoms in Nepalese CL wearers is expected. Such symptoms should be addressed in time for continuous efficient CL wear. Nepalese soft CL wearers, especially with low compliance rate, were found at high risk of developing ocular complications due to high CL case and solution contamination.12 In a large sample size study recently conducted in Nepal, we found ocular complications in about 5% of the total soft CL wearers including microbial keratitis in 3% eyes.10
There is not any standard protocol regarding ocular symptoms of CL wearers. Some researchers considered few symptoms while others included a large number of symptoms in their studies.13,14 Some researchers have graded each symptom into four grades depending upon the frequency of symptoms.13
To the authors’ knowledge, no study has been conducted in Nepal regarding symptoms associated with CL wear. The purpose of this pilot study was to find the common ocular symptoms in Nepalese soft CL wearers. The results of this study may be helpful to address the causes of CL discontinuation and to improve quality of life of Nepalese CL wearers. Also the findings of this study might be helpful in future studies in symptoms in soft CL wearers in this region.
MethodsA cross-sectional study was conducted including all the current soft CL wearers who started to wear CL from Nepal Eye Hospital (NEH) between July 2007 and June 2012 (five year period). NEH is one of the four tertiary eye hospitals located in Kathmandu which is the most populated and polluted city of Nepal.11 Besides the general patients, people wishing to wear CL as well as patients referred by other eye care practitioners for specialty CL (e.g. keratoconus, scleral) visit NEH. Eye care practitioners fit lenses in suitable candidates after eye examination including refraction, slit lamp examination, keratometry and tear film assessment. A leaflet with written guidelines is provided for each CL wearer about the care and maintenance. Briefly, it contains information about insertion and removal procedure, proper handling methods. Patients are also advised about wearing hours per day, wearing days per week, lens replacement schedule and follow-up visit according to the prescribed type of lens and/or the ocular health of the subjects. CL wearers from NEH only were included to homogenize the guidelines presented to the participants about the handling and maintenance of CL. Subjects who were wearing CL with a purpose other than refractive error correction were excluded from this study.
A standard proforma was developed to obtain demographic information e.g. age, sex, type and regimen of CL, lens care system, duration of wear, wearing hours/day, number of wearing days/week, profession and any active or passive cigarette smoking. Ten ocular symptoms (uncomfortable CL, blurring vision, redness, itching, watering, dryness, foreign body sensation, reduced wearing time, burning and headache), commonly found in CL wearers, were included in the questionnaire.
Each symptom was classified in four levels of frequency: never, occasionally, frequently and consistent and scored as 0, 1, 2 and 3, respectively.13 The questionnaire was filled out by a masked optometrist who was unknown about type of CL and care system used by the subjects. The final symptom score was calculated by adding up the scores of ten symptoms, thus the symptom score could be in the range of zero to thirty.
Ethical approval was provided by Institutional Review Board of Nepal Netra Jyoti Sangh. Each subject signed on a consent form containing details about the study in local language. This study followed the tenets of Declaration of Helsinki. Health Insurance Portability and Accountability Act 1996 regulations were followed for all of the study participants.
Data were analyzed using the statistical package SPSS 21 statistical software (SPSS Inc., Chicago, IL, USA). A normal distribution of variables was assessed using Kolmogorov–Smirnov test. Parametric tests were applied in normally distributed variables and non-parametric tests for others. Association between the degree of symptoms with the maintenance solution, sex, cast, education, profession and passive smoking were studied with Mann–Whitney test. Correlation of symptom score with quantitative variables (age, wearing hours per day, wearing days per week and CL power) was determined with Spearman correlation. p value less than 0.05 was considered as statistically significant.
ResultsTwo hundred and three subjects, who were wearing soft CL, were informed and requested to participate in the study. Out of them, 63.6% (129) participated and were included in this study. The majority of the participants (95%) were wearing conventional lenses with the remaining wearing monthly disposable lenses. Eighty six percent of the subjects were from urban areas. None of the subjects was wearing lens in extended wear regimen. Sixty seven percent (n=87) of the subjects were female. All of the subjects were using multipurpose solution (MPS) for lens care: 53.5% using Renu Multiplus MPS (Bausch and Lomb, Rochester, NY), 17.8% Opti-Free Express MPS (Alcon Laboratories, Inc., TX), 14% Purcon-Puresoft MPS (Purecon Lenses Pvt. Ltd., New Delhi, India) and remaining 14.7% either unknown or brand name not leveled in the bottle. Demographic information is shown in Table 1.
Demographic data of the study subjects.
| Age (±SD) | 23.9±4.28 years (range: 15–39 years) |
| Gender (N=129) | |
| Male | 42 (33%) |
| Female | 87 (67%) |
| Ethnicity (N=129) | |
| Newars | 53 (41.1%) |
| Brahmin | 35 (27.1%) |
| Chhetriyas | 26 (20.2%) |
| Others | 15 (11.6%) |
| Education (N=129) | |
| Under Grade 10 | 3 (2.3%) |
| Grade 10–12 | 40 (31.0%) |
| Graduated | 86 (66.7%) |
| Profession (N=129) | |
| Non medical | 100 (77.5%) |
| Medical | 29 (22.5%) |
| Passive smoker (N=129) | |
| Yes | 31 (24.0%) |
| No | 98 (76.0%) |
| Contact lens power | −3.30±3.06 D |
| Duration of lens wear | 2.81±2.32 years (range: 1–6 years) |
| Wearing hours per day | 9.76±2.93 (3–18) |
| Wearing days per week | 5.88±1.48 (2–7) |
Minimum of one symptom was found in 96.9% of the subjects at least occasionally. The average number of symptoms was 5.9±2.2 (range: 0–10) with mode 6.
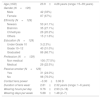
Fig. 1 shows the average score of each symptom. The frequency of the different symptoms found in the study is summarized in Fig. 2. Eighty eight percent (n=114) of the subjects had symptoms of discomfort during their lens wearing time. However, 73.6% of the subjects felt discomfort occasionally. Other commonly found symptoms were foreign body sensation in 73.6% (n=95), redness in 65.9% (n=85), reduced wearing time in 63.6% (n=82) and dryness of eyes in 62.8% (n=81) of the total subjects. Blurring vision was found in 59.7% (n=77), watering in 58.1% (n=75), itching in 42.6% (n=55) and burning in 41.1% (n=53). Headache was found to be the least common symptom comprising 36.4% (n=47) of the subjects. Symptoms were found occasionally in the majority of the subjects. Consistent symptoms were found in rare cases; for instance: consistent reduced wearing time in 8.5% (n=11) and consistent blurring vision in 0.8% (n=1).
![Mean score of each symptom, error bar representing the 95% CI of mean score [CL – contact lens; FBS – foreign body sensation].](https://static.elsevier.es/multimedia/18884296/0000000800000003/v2_202107280542/S1888429615000059/v2_202107280542/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w93meMsSv3kCFu9ka1kgzl/xrK32s3f4YRcWD6Dd7AXar8ukQFMuybRxJvMissAAPsYxFDkr/buoy7sFNIne2wY30HvTQYyWLkIvEVbYCzNmjXLfz8eX1jC5vJjZWMpEoVTa+NJrd4+0zsTPj3xnZ8p1B57IMsijOxJvbVnlbslCZb3I/ke8khox542My+XCu2QPv55rytksOlTTHnB9SQjoH4DsNlmVskGE3O1luNmEYtt0sW9HIA4eZoUzCP2Dy3A== "Mean score of each symptom, error bar representing the 95% CI of mean score [CL – contact lens; FBS – foreign body sensation].")
![Frequency of symptoms of the participants [CL – contact lens; FBS – foreign body sensation].](https://static.elsevier.es/multimedia/18884296/0000000800000003/v2_202107280542/S1888429615000059/v2_202107280542/en/main.assets/gr2.jpeg?xkr=ue/ImdikoIMrsJoerZ+w93meMsSv3kCFu9ka1kgzl/xrK32s3f4YRcWD6Dd7AXar8ukQFMuybRxJvMissAAPsYxFDkr/buoy7sFNIne2wY30HvTQYyWLkIvEVbYCzNmjXLfz8eX1jC5vJjZWMpEoVTa+NJrd4+0zsTPj3xnZ8p1B57IMsijOxJvbVnlbslCZb3I/ke8khox542My+XCu2QPv55rytksOlTTHnB9SQjoH4DsNlmVskGE3O1luNmEYtt0sW9HIA4eZoUzCP2Dy3A== "Frequency of symptoms of the participants [CL – contact lens; FBS – foreign body sensation].")
Total symptom score was less than 10 in four fifths of the subjects and less than 20 in 99% of the subjects.
As shown in Table 2, symptom score was not correlated or associated with other factors like age, sex, education status, ethnicity and profession of the subjects, maintenance solution used, duration of lens wear, number of lens wearing hours per day, number of lens wearing days per week and lens power (p>0.05). However, it was highly associated with the passive smoking (p<0.001).
Relationship of symptom score with different factors.
| Association of symptom score with different variables | |
|---|---|
| Variables | p values |
| Solution types | 0.872 |
| Gender | 0.888 |
| Ethnicity | 0.263 |
| Education | 0.266 |
| Profession | 0.111 |
| Passive smoker | <0.001 |
| Correlation of symptom score with different factors | ||
|---|---|---|
| Variables | r values | p values |
| Age | 0.023 | 0.794 |
| Duration of lens wear | 0.012 | 0.890 |
| Wearing hours a day | −0.100 | 0.260 |
| Wearing days a week | −0.049 | 0.579 |
| Lens power | 0.079 | 0.156 |
This study highlights the common symptoms in current soft CL wearers in Nepal and its association with other factors. All the current soft CL wearers who commenced wearing CL from the NEH were informed for the participation in this study. We found the response rate to be 63.6%, which is comparable to other studies.15,16
Our study revealed that almost all (96.9%) of the soft CL wearers in Nepal suffer from some types of symptoms during some period of CL wear. Symptoms varied in extent from occasionally to consistently and single to multiple. Our findings support the results of recent studies conducted in Nepal. Panthi et al. concluded that Nepalese soft CL wearers are at higher risk of developing ocular complications and of contamination of lens care accessories.12 In our previous study, we found high prevalence of microbial keratitis (0.15% of total 4064 subjects) in Nepalese soft CL wearers.10 In the current study, the prevalence rate of symptoms was higher compared to the rate of symptoms in other studies. Doughty et al. found some kind of symptoms in 78.5% of the soft CL wearers.13 Average number of symptoms found in our study was also higher than that of their study (6 versus 1.49). The main reason behind the high rate of symptoms of Nepalese CL wearers may be the high dust and smoke pollution of the city areas.11 Another reason may be due to improper lens care system. Although all the subjects were using MPS for lens clean and soak, 14% were using Purecon-Puremoist (EDTA 0.1%), which does not contain any appropriate disinfectant and 14.7% were using either unknown or solution without any brand name. Most of the previous studies considered only few symptoms such as discomfort and dryness. In this study, we included ten different symptoms. Almost all of these CL wearers had suffered from one of these symptoms at some period of time. Moreover, the majority of the participants had worn conventional lenses with low Dk materials, which can also contribute to this number.5 Most of the symptoms were found occasionally so that these subjects were still wearing CL. Low compliance, improper fittings of CL might also be the contributing factors for the high rate of symptoms. But as far as we know, no studies about the compliance rate and the fitting status have been conducted in Nepalese CL wearers.
This study showed that discomfort, foreign body sensation, redness, reduced wearing time and dryness are the five most common symptoms found in soft CL wearers in this region. Similar to the results of Begley et al. more than four fifths of the total participants gave history of discomfort during the lens wearing time.17 However, the majority of the subjects in our study felt discomfort occasionally.
Scratchiness was the second most common symptom, which was present in 74% of the subjects. It was found frequent and consistent in 12% of the subjects. Still it was higher than that of the study by Riley et al. where only 7% of the CL wearers had frequent or constant foreign body sensation symptom.5 Reasons of foreign body sensation in CL wearers may be improper lens fittings/designs, dry eyes or dust/smoke pollution in our cases. Another factor contributing to this feeling may be the adsorption of deposits. Since in our study the majority of the subjects were wearing conventional lenses, the amount of deposits might be higher.18
Two thirds of the subjects had redness of eyes during CL wear and it was found to be the third most common symptom. Similar to our finding, Jones et al. also found redness in 36–41% of the CL wearing subjects.19 Redness of eyes with CL may be due to dry eyes, ocular allergy, and solution sensitivity or due to the hypoxia in low Dk lens wearers. Reduced wearing time was found in 64% of the participants and 60% of them had occasional problems. Reduced wearing time may be due to reduction in comfort after few hours of lens wear.20
We found dryness in 63% of the subjects. Similar to our finding, Jones et al. also found dryness in 50–65% of their CL wearers.19 The etiology of dry eyes is multi-factorial and is one of the main causes of lens drop out.9
Although almost all the cases showed some type of symptoms, majority of them had occasional symptoms. Eighty percent of the subjects had symptom score less than 10 and 99% had less than 20. This indicates why these patients are still wearing CL, though they have symptoms.
Panthi et al.12 found different contamination rates with different lens care solutions used in Nepal. This result could suggest different risk to microbial adverse effect related with different CL care system, but we did not find statistically significant association between symptom score and lens care system used. Degree of symptoms was not found to be associated with age, sex, education, profession and duration of CL wear. Similar symptom scores were found in: male and female, high educated or low educated, and medical person or non-medical person. Similarly, symptom score was found similar with respect to the number of lens wearing hours per day or wearing days per week. It is surprising that symptom score was not associated with the duration of CL wear. These findings are consistent with a study conducted by Brennan and Efron in conventional lens wearers.21
In this study, none of the subjects was smoker. However, degree of symptoms was found to be highly associated with the exposure to passive cigarette smoke. CL wearers, who share home with smoker, were found to have higher symptom score. This might be due to the fact that passive exposure to cigarette smoke increases the tear inflammatory cytokines, tear lipid peroxidation products and decreases the mucosal defense resulting tear instability and damage the ocular surface epithelia.22
There are some limitations of the study. We only considered the frequency of the symptoms but not their intensity. We included only the current CL wearers. Those people, who discontinued CL wear due to symptoms, were not included; that could change the rate of symptoms. We limited our study within ten symptoms, so this study may not be comparable to the other studies that included different number of symptoms. Future studies with standardized questionnaires are necessary. Different study set-up, variation in the study subjects and materials and inclusion of occasional symptoms may be the reasons behind different findings with many other studies.
From this study, we can conclude that almost all the soft CL wearers in this region had symptoms during some time period of lens wear. The common symptoms were discomfort, foreign body sensation, redness, reduced wearing time and dryness, which are the main causes of CL discontinuation. Many CL wearing patients are still continuing the CL because most of them have these symptoms occasionally. CL practitioners in this region are recommended to prescribe high oxygen permeable silicone CLs, preferably with frequent disposable regimen. With application of proper lubricating eye drops and protection from dust and smoke, symptoms may be reduced.
Conflicts of interestThe authors have no conflicts of interest to declare.
Source of fundingNone.
This study was presented (orally) in 19th Asia Pacific Council of Optometry, 2013, Seoul, Korea. The presentation was supported by Fellowship of World Council of Optometry. Authors would like to thank Ms. Bijaya Pandit and Mr. Michael J. Rosenkrantz for their help in data collection and manuscript preparation.





