




To investigate the influence of offsets of the pupil center from the corneal vertex on wavefront aberrations in the anterior cornea and the whole eye.
MethodsBoth right and left eyes of 103 subjects were measured for the wavefront aberrations in the anterior cornea, along with the offset of the pupil center relative to the corneal vertex, using a Humphrey corneal topographer, and for the wavefront aberration in the whole eye using a WASCA wavefront sensor. Correlations of the pupil center offsets with the Zernike aberrations were tested.
ResultsX-axis shift of the pupil center from the corneal vertex was significantly correlated to horizontal coma for both the right (r = 0.54, P<0.0001) and left eyes (r=0.48, P<0.0001) in the cornea, but was weakly correlated to the coma in the whole eye (r=0.17, P=0.04 for OD; and r=0.17, P=0.05 for OS). Significant but weak correlations with the x-axis pupil center shift were also found for several other Zernike aberrations, including the oblique astigmatism, vertical trefoil and secondary astigmatism. Very few Zernike aberrations were significantly correlated to y-axis pupil center shift. Most Zernike aberrations were significantly correlated between the right and left eyes to produce bilateral symmetry in the cornea and the whole eye.
ConclusionsThe results suggest that offset of the pupil center from the corneal vertex plays an important role in determining horizontal coma and few other Zernike aberrations. Factors controlling bilateral symmetry of the wavefront aberrations between the two eyes could make important contributions to wavefront aberrations in the human eye.
Investigar el efecto que tiene el descentramiento de la pupila con respecto al vértice corneal sobre las aberraciones del frente onda asociadas tanto a la cara anterior de la córnea como a la totalidad del ojo.
MétodosEn los ojos derecho e izquierdo de 103 sujetos se midieron las aberraciones del frente de onda asociadas tanto a la cara anterior de la córnea (utilizando un topógrafo corneal Humphrey), como a la totalidad del ojo (utilizando un sensor de frente de onda WASCA). Asimismo, se midió el desplazamiento del centro de la pupila respecto a la posición del vértice corneal, utilizando el mismo topógrafo corneal Humphrey anteriormente mencionado. Se investigó la posible correlación entre el valor del desplazamiento del centro de la pupila y los distintos términos de aberraciones de Zernike.
ResultadosEl desplazamiento según el eje x del centro de la pupila respecto al vértice corneal muestra una correlación significativa con el valor del coma horizontal en la córnea tanto para los ojos derechos (r=0,54; P<0,0001) como para los izquierdos (r=0,48; P<0,0001); sin embargo, existe una correlación muy débil entre el valor de este desplazamiento y el coma de toda la óptica ocular (r=0,17; P=0,04 para OD; y r=0,17; P=0,05 para OI). También se obtuvieron correlaciones débiles aunque significativas entre el desplazamiento del centro de la pupila en el eje x y otros coeficientes de aberración de Zernike, entre los que se incluye el astigmatismo oblicuo, el astigmatismo triangular (trefoil) y el astigmatismo secundario. Muy pocos tipos de aberración (términos de Zernike) presentaron una correlación significativa con el desplazamiento del centro de la pupila en el eje y. También se encontró una correlación significativa para la mayoría de los términos de aberraciones (coeficientes) de Zernike entre el ojo derecho y el izquierdo de un mismo individuo, de tal forma que daba lugar a simetría bilateral tanto en la córnea como en la totalidad del ojo.
ConclusionesLos resultados sugieren que el descentramiento de la pupila con respecto al vértice corneal tiene una notable influencia sobre el valor del coma horizontal y de algunas otras aberraciones de Zernike. Los factores que controlan la simetría bilateral entre ambos ojos (en lo que respecta a la aberración del frente de onda) podrían suponer una contribución importante a las aberraciones del frente de onda del ojo humano.
Understanding the sources of wavefront aberrations in the human eye is important not only for scientific research but also for the clinical practice since it could provide basic information about the eye for studying optical nature of the eye and also for guiding accurate wavefront diagnosis and correction. Wavefront aberrations of the eye are measured with respect to the line of sight, formed by the line joining the fixation point and the centre of the entrance pupil.1 Thus, optical axes of the refractive surfaces of the cornea and the lens should be all coincident to the line of sight in order to minimize wavefront aberrations in the eye. But, this is not the case for most of our eyes.
The anterior corneal surface, as the most important optical part in determining the refractive power and wavefront aberrations of the eye, is usually decentered and tilted with respect to the line of sight. Its axis with respect to the pupil center, the pupillary axis, forms an angle with the line of sight that is the angle lambda. Given an angle lambda in the eye, the optical performance of the anterior cornea, relative to the line of sight, is just like eccentrically imaging an off-axis visual target, and therefore, it must produce asymmetric aberrations as those demonstrated in recent wavefront measurements for the peripheral field.2-5 It is therefore interesting to test how and to what extent the angle lambda influences wavefront aberrations in normal population.
In order to accomplish the task, we would require measurements on both angle lambda and wavefront aberrations for every subject. Fortunately, most corneal topography systems used to measure corneal wavefront aberrations provide at the same time an indirect estimate of the angle lambda. In corneal topography, the corneal vertex, defined as the intersection of keratometric axis with the anterior corneal surface and located at the center of corneal topography maps, is usually not at the center of the apparent pupil. The offset of the pupil center from the corneal vertex was found to be highly correlated with the angle lambda,6-7 thus giving rise to an indirect estimate of the angle lambda. It is therefore practical to test the influence of angle lambda on wavefront aberrations using the offset between the corneal vertex and the pupil center obtained from the corneal topography measurements. In this study we have measured offset of the pupil center from the corneal vertex and wavefront aberrations in the anterior corneal surface as well as in the whole eye for a group of 103 young normal subjects.
MethodsSubjectsIn this study, one hundred and three subjects (fifteen emmetropes and eighty eight myopes) were recruited among the college students of the Wenzhou Medical College and the candidates for refractive surgery in the Refractive Surgery Center of Eye hospital, Wenzhou Medical College, China, with a mean age of 25.1±4.6 years (range 18 to 38 years). The mean spherical equivalent refractive errors for the emmetropes was -0.06±0.24D (range -0.38 to 0.38D) for OD and 0.06±0.31D (range -0.38 to 0.63D) for OS. The myopic subjects had mean spherical equivalent refractive errors of -5.1±2.1D (range -10.0 to -0.65D) for OD and -5.1±2.1D (range -10.0 to 0.38D) for OS. Subjects with any ocular pathology or with astigmatism greater than 2.5 D were excluded. The best-corrected visual acuity for this group of subjects was 20/25 or better. The research followed the tenets of the Declaration of Helsinki with informed consent signed by all of the subjects, and was approved by the Committee of Ethics of Wenzhou Medical College.
Instruments & Experimental ProcedureTwo instruments, a Humphrey ATLAS Corneal Topography System (Carl Zeiss Meditec Inc, Jena, Germany) and a WASCA Wave-front Analyzer (Carl Zeiss Meditec, Germany), were used to measure wavefront aberrations in the cornea and in the whole eye. The ATLAS system directly provides estimates of the corneal vertex, pupil margins, pupil center location, shape factor, curvatures of the anterior corneal surface, and keratometric measurements. But the accuracy on the estimation of the pupil margin and pupil center was suspect for some subjects. In order to accurately estimate the pupil margin and the pupil center, we have developed a MatLab program to process the raw images, directly exported from the ATLAS system. The pupil size derived from our own image processing was then compared to that from the ATLAS software. If the difference of pupil sizes between the two estimates was less than 0.5mm, we believed that the estimates of pupil margin and hence the pupil center by the ATLAS system were accurate. Otherwise, we treated the ATLAS estimates as inaccurate, and excluded the subject from further data analysis. Meanwhile, we excluded subjects with a pupil size <4.0mm and >5.0mm in order to minimize the influence of pupil size on pupil center location. The corneal curvature and corneal height data were used to derive corneal aberrations, and the distance of the pupil center relative to corneal vertex in both horizontal and vertical directions were directly measured with scale ruler in the corneal topography mapin order to assess the pupil center offset.
The WASCA Wave-front Analyzer was used to measure wavefront aberrations for the whole eye. The system directly provides refractive error and a series of Zernike aberrations.
For each subject, we have obtained three measurements of corneal topography, without data missing in a 6.00mm central area, and three measurements of wavefront aberrations in the whole eye. Room light was off during the aberration measurement for the whole eye, pupil sizes were at least 6.00mm for all of the subjects included in this study. Both right and left eyes for each subject were tested, and in total, data collection took about 15minutes.
Data AnalysisFor each corneal measurement, Zernike aberrations up to 7th order (35 terms) were calculated using a customized MatLab ray-tracing program8-9 from the height data exported from the ATLAS system. The data of corneal heights within a 4.5mm corneal central area were calculated, and the Zernike aberrations in the whole eye within a 4.5mm central pupil area were obtained by reprocessing the WASCA data. In order to make the corneal aberrations to be centered with the line of sight of the eye, as for the whole eye aberrations, correction of displacement between corneal vertex and pupil center was performed in the customized program, using the measurements of the pupil center from the ATLAS system. For both the anterior cornea and the whole eye, a mean of three measurements was used to estimate the Zernike aberrations for each eye. We used the single-index conversion for naming the Zernike aberrations recommended by the OSA/VSIA Standards Taskforces.1 Pupil center offset for each eye was calculated from a mean of three measurements from the corneal topographies. Figure 1 shows the corneal axial power maps of the right eye for two subjects (a+c) and the corresponding wavefront aberration maps for a 4.5mm pupil area in the whole eye (b+d). Difference in the offset of pupil center from the corneal vertex between the two subjects can be found from Figure 1a and c. All statistical regression analyses were performed using SPSS 13.0 (SPSS Inc., Chicago, IL, USA), and a t-test was used to compare differences of mean aberrations between the right and left eyes.
ResultsOffset of the Pupil Center with the Corneal Vertex and Its Correlation with Zernike Aberrations and wavefront aberration maps over a 4.5 mm pupil area (b+d) for two subjects. The corneal maps are centered at the corneal vertex with the cross indicating the pupil center.")
Mean horizontal shifts of the pupil center for the 103 normal eyes were -0.05±0.08 and 0.02±0.10mm for the right and the left eyes respectively, and the difference was significant (t= 5.38, P<0.0001). But no significant difference between the right (0.02±0.07mm) and left eyes (0.04±0.08mm) was found for the vertical pupil center shifts.
Individual offsets of the pupil center with corneal vertex for the 103 subjects are illustrated in figure 2 for both the xaxis (red circles) and y-axis (green circles) directions. As shown in figure 2, the pupil centers tended to shift horizontally in opposite direction between the right and left eyes, resulting in a negative correlation (r=-0.52, P<0.0001, red line). But the vertical shifts were in the same direction for the both eyes, with a positive correlation (r=0.50, P<0.0001, green line).
 and vertical directions (green circles) for the 103 subjects, with the solid and dashed lines representing regression lines.")
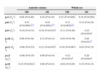
Correlations between the pupil center shifts and the Zernike aberrations over a 4.5mm pupil area were analyzed separately for the right and left eyes. Table 1 summarizes the correlation coefficients (for the x-axis direction) for those Zernike aberrations for which at least one coefficient was statistically significant out of the four correlations (x-axis pupil center shifts vs. corneal aberrations in OD and OS and whole eye aberrations in OD and OS). Correlations for Zernike aberrations beyond 5th order were not listed in the table 1 because the aberrations were very small in magnitudes. As shown in the table 1, there were 7 terms among the 18 Zernike aberrations from 2nd to 5th order por which at least one correlation was statistically significant. Horizontal coma was the one that had more of significant coefficients (three out of four) and also higher coefficient values (all above 0.3) among the 7 terms. For the horizontal coma, the coefficients in the cornea were greater than in the whole eye. Figure 3 shows the correlations between the x-axis pupil center shift and horizontal coma in the right (the red circles and red lines) and the left eyes (the green circles and green lines) for the 103 subjects in the anterior cornea (a) and the whole eye (b). For the other Zernike terms, the coefficients were low, less than 0.3. The vertical trefoil (j=9) for both the anterior cornea and the whole eye was negatively correlated to x-axis pupil center shift, but that in the left eye was statistically significant. The secondary astigmatism (j=13) was significantly correlated to x-axis pupil center shift in the whole eye, but not in the anterior cornea.
Correlation between Zernike aberrations over a 4.5 mm pupil area and offsets of the pupil center from the corneal vertex in both the anterior cornea and the whole eye for 103 normal subjects.
| Anterior cornea | Whole eye | |||
| OD | OS | OD | OS | |
| j=3 (Z2-2) | 0.08 (P=0.40) | 0.16 (P=0.10) | 0.22 (P=0.026)* | 0.19 (P=0.059) |
| j=8 (Z31) | 0.51 (P<0.0001)*** | 0.42 (P<0.0001)*** | 0.31 (P<0.0025)** | 0.12 (P=0.24) |
| j=9 (Z33) | -0.10 (P=0.31) | -0.24 (P=0.015)* | -0.11 (P=0.26) | -0.21 (P=0.034)* |
| j=10 (Z4-4) | 0.09 (P=0.38) | 0.15 (P=0.14) | -0.03 (P=0.76) | 0.26 (P<0.01)** |
| j=11 (Z4-2) | -0.06 (P=0.53) | -0.21 (P=0.033)* | -0.18 (P=0.067) | 0.03 (P=0.73) |
| j=13 (Z42) | -0.09 (P=0.35) | 0.09 (P=0.34) | -0.21 (P=0.033)* | 0.20 (P=0.043)* |
| j=18 (Z51) | 0.23 (P=0.021)* | 0.08 (P=0.43) | -0.02 (P=0.85) | 0.15 (P=0.13) |
Statistical Significance
 and the left eye (green circles) in (a) the cornea and (b) the whole eye, with the solid and dashed lines representing regression lines.")
For y-axis pupil center offset, only three Zernike terms were significantly correlated, including the whole-eye defocus (j=4) in both the right (r=0.35, P<0.001) and left eyes (r=0.25, P<0.01), the whole eye spherical aberration (j=12) in the left eye (r=0.24, P=0.015), and the whole eye secondary trefoil (j=16) in both the right (r=0.24, P=0.14) and left eyes (r=0.24, P=0.15). None of the Zernike aberrations in the anterior cornea was significantly correlated to y-axis pupil center shift.
Correlation of Zernike Aberrations between the Two EyesFor the group of 103 normal subjects, correlations of Zernike aberrations between the right and left eyes in both the anterior cornea and the whole eye were also tested, and are depicted in table 2, where only the aberrations from 2nd to 5th order (18 terms) are listed. Some of the Zernike aberrations are marked with asterisks indicating statistical significance of the correlation after corrected for multi-comparison. Among the 18 Zernike terms, eight aberrations (including j=3, 8-11 and 18-20) are asymmetrical to y-axis of the pupil, and the correlations of these aberrations are all negative and significant, except j=11 in the anterior cornea and j=19-20 in both the anterior cornea and the whole eye. For the other Zernike aberrations (j=4-7, and 12-17) symmetrical to y-axis of the pupil, the correlations were all positive and significant, except of the corneal j=15.
Correlation coefficients of Zernike aberrations over a 4.5 mm pupil area between the right and left eyes for 103 normal subjects.
| Anterior cornea | Whole eye | |||
| r | p | r | p | |
| j=3 (Z2-2) | -0.60*** | <0.0001 | -0.45*** | <0.0001 |
| j=4 (Z20) | 0.36*** | <0.001 | 0.94*** | <0.0001 |
| j=5 (Z22) | 0.89*** | <0.0001 | 0.85*** | <0.0001 |
| j=6 (Z3-3) | 0.65*** | <0.0001 | 0.59*** | <0.0001 |
| j=7 (Z3-1) | 0.85*** | <0.0001 | 0.75*** | <0.0001 |
| j=8 (Z31) | -0.57*** | <0.0001 | -0.50*** | <0.0001 |
| j=9 (Z33) | -0.52*** | <0.0001 | -0.41*** | <0.0001 |
| j=10 (Z4-4) | -0.33*** | <0.001 | -0.22* | 0.028 |
| j=11 (Z4-2) | -0.11 | 0.26 | -0.24* | 0.017 |
| j=12 (Z40) | 0.53*** | <0.0001 | 0.85*** | <0.0001 |
| j=13 (Z42) | 0.64*** | <0.0001 | 0.42*** | <0.0001 |
| j=14 (Z44) | 0.32*** | <0.001 | 0.43*** | <0.0001 |
| j=15 (Z5-5) | -0.13 | 0.20 | 0.09 | 0.35 |
| j=16 (Z5-3) | 0.24** | 0.016 | 0.61*** | <0.0001 |
| j=17 (Z5-1) | 0.42*** | <0.0001 | 0.36*** | <0.001 |
| j=18 (Z51) | -0.10* | 0.33 | -0.21* | 0.037 |
| j=19 (Z53) | 0.04 | 0.68 | -0.01 | 0.89 |
| j=20 (Z55) | -0.04 | 0.70 | -0.12 | 0.21 |
We have measured offset of the pupil center from the corneal vertex and wavefront aberrations in both the anterior corneal surface and the whole eye over a 4.5mm pupil area for 103 normal subjects in this study. The mean offsets of the pupil center for this group of subjects showed a general mirror symmetrical pattern between the right and left eyes, with negative x-axis shift in the right eye and positive shift in the left and, at the same time, positive y-axis shifts for the both eyes. The mirror symmetrical patterns also holds for individual subjects, since the offsets were negatively correlated between the right and left eyes for the x-axis shift and positively correlated for the y-axis shift (Figure 2). Another characteristic of the pupil center offset for this group of subjects was the substantial individual variations, and it covered about a range of 0.5mm for the x-axis shift and 0.4mm for the y-axis shift (Figure 2).
Given the substantial individual variation of the pupil center shifts in this normal population, it is possible to explore the contribution of the pupil center offset from the corneal vertex to wavefront aberrations in normal eyes by testing their relationship. We found that the horizontal coma was significantly correlated to the pupil center shift in both the anterior cornea and the whole eye, but the correlations in the whole eye were weaker compared to the cornea. The results indicate that the offset of the pupil center from the corneal vertex, hence the angle lambda in x-axis direction, plays an important role in determining the horizontal comas in the cornea and in the whole eye, and that the reduced influence of the pupil center shift on the whole eye horizontal coma is probably due to an angle-lambda-linked compensation from the internal optics. This is in agreement with several recent studies on compensation of horizontal coma between the anterior cornea and internal optics.10-11 This is also consistent with the theoretical account on relationship between spherical aberration and coma aberration in a previous study.12 But, surprising to us was the non-significant correlations between the y-axis pupil center shift and the vertical coma. This result implies that the vertical coma is not mainly determined by the pupil center shift and therefore must be dependent on other factors. For example, intraocular pressure was recently found to be related to vertical coma.9 Studies on the effects of reading on corneal aberrations also revealed that the eye lid pressure could change the vertical coma as well as the trefoil.13
Besides the coma aberration, weak but significant correlations were found for several other Zernike aberrations. The oblique astigmatism in the whole eye was significantly correlated to x-axis pupil center shift in the right eye and was on the border of significance in the left eye. Dependency of the oblique astigmatism on eccentric degree has been demonstrated in several previous measurements of the peripheral wavefront aberrations.2-5 Results in this study were consistent with the previous studies, but with weaker effects probably because the x-axis pupil center shifts, hence the eccentric degrees, for our normal subjects were very limited. Meanwhile the effect of the pupil center shift on astigmatism in this study was observed only on x-axis for our normal subjects, and no significant correlation was found between the y-axis pupil center shift and Zernike astigmatisms. The results could further imply that the vertical aberrations might be affected by multiple factors, and thus the effect of y-axis pupil shift was masked.
All correlations between the x-axis pupil center shifts and vertical trefoils (j=9) in the cornea and the whole eye were negative, contrary to the positive correlations found for the horizontal coma, even though the correlations were not statistically significant in the cornea. It is very possible that the influence of the x-axis pupil center shift on the trefoil was linked to the horizontal coma, just like the influence of the eyelid on both the coma and trefoil during reading.13
From this study, it seems very likely that the offset of x-axis pupil center from the corneal vertex plays a more important role in determining the wavefront aberration in the normal eyes than the y-axis pupil center shift since more terms of the Zernike aberrations were related to the x-axis pupil center shift. Yet, it is true that the x-axis pupil center shift covers a wider range than the y-axis shift, therefore, stronger effect would be expected for the x-axis shift than the y-axis shift. However, the difference in the ranges between the two directions of the pupil center shifts was only about 20%, so it might not be enough to explain the big differences that we observed in this study. Thus, factors other than the pupil center shift might play more important role in determining the vertical aberrations than the horizontal aberrations.
Manipulation on optical system of the eye is widely practiced to treat eye problems in both optometric and ophthalmologic areas, such as contact lenses, intra-ocular lens and laser corneal ablation. Any type of treatment could change the optical structure of the eye and consequently introduce new relationship between the pupil center and the line of sight. It is therefore interesting to ask if the conclusions on relationship between Zernike aberration and pupil center offset derived in this study from our normal subjects will still hold for the clinical cases. While definite answer to the question will rely on further experimental measurement, it might be reasonable to expect that the conclusions will still hold if the extent of pupil center offset under the clinical conditions was not too much over the range as reported in this study for normal subjects.
Bilateral symmetry of wavefront aberrations between the right and left eyes in both the anterior cornea and the whole eye was well documented,14-21 even though the mechanisms underlying the bilateral symmetry were poorly understood. The necessary condition for bilateral symmetry of wavefront aberrations between the two eyes is that the Zernike aberrations in the right and left eyes should be about the same amplitude and with opposite sign for those Zernike terms which are asymmetrical about the vertical axis of the pupil (such as the oblique astigmatism j=3 and the horizontal coma j=8), but with the same sign for those terms which are symmetrical about the vertical axis of the pupil (such as main-axis astigmatism j=5 and vertical coma j=7). For a group of subjects, the aberrations of each Zernike term should be correlated to each other between the two eyes positively or negatively, depending on whether the Zernike term is asymmetric or symmetric about the the y-axis of the pupil. In this study we have shown that the correlations of Zernike aberrations between the right and left eyes were significant for most of the 2rd to 5th order Zernike terms (Table 2), and the correlations were in the right directions for bilateral symmetry. The results thus confirmed the bilateral symmetry of the wavefront aberrations in both the anterior cornea and the whole eye, as found in previous studies.14-21
While most of the Zernike aberrations have showed strong correlations between the two eyes, the correlations between the Zernike aberrations and the pupil center offsets were much weaker and for only few terms. This means that factors controlling the bilateral symmetry of wavefront aberrations between the two eyes play a more important role in determining wavefront aberrations in the normal eyes than the factor of pupil center shift. It is therefore worthwhile to study bilateral symmetry of the wavefront aberrations further.
In summary, the offset of the pupil center from the corneal vertex was found to be significantly correlated to horizontal coma and few other Zernike aberrations for our 103 normal subjects, and the results imply that the pupil center offset plays an important role in causing horizontal coma and few other aberrations. Meanwhile, the strong correlations of Zernike aberrations between the right and left eyes suggest that factors controlling bilateral symmetry of wavefront aberrations between the two eyes could play more important roles in determining the wavefront aberrations in the human eye.





