


There have been numerous and extensive studies into the visual requirements for reading in adults with low vision. There are far fewer studies involving children with low vision. This article compares the studies on children which do exist with the findings in adults. Acuity reserve (magnification), contrast reserve and visual field requirements are considered. We also review the literature which compares the efficacy of large print with optical magnification for children. From the few studies that exist, there are indications that the requirements for children are not the same as for adults. Therefore, we suggest that one cannot directly apply the results from adults to children and that there is a gap in the literature (and therefore our understanding) of the visual requirements for reading in children.
Se han publicado numerosos y extensos estudios sobre las necesidades visuales de lectura en adultos con baja visión. Se dispone de un número mucho menor de estudios en niños con este problema. En el presente artículo se comparan los estudios disponibles efectuados en niños con los hallazgos identificados en adultos. Se consideran la reserva de agudeza (magnificación), la reserva de contraste y las necesidades de campo visual. También se revisan los estudios publicados que comparan la eficacia de los textos impresos con letra grande con la magnificación óptica para niños. A partir de los estudios existentes, hay indicaciones de que las necesidades para niños no son iguales que para los adultos. Por esta razón, sugerimos que no se apliquen directamente los resultados de adultos a los niños y consideramos que se requiere un mayor número de estudios (y, por lo tanto, nuestros conocimientos son incompletos) sobre las necesidades visuales de la lectura en niños.
Visual impairment is a globally prevalent issue in both adults and young populations. According to World Health Organization (WHO),1 in 2002 there were more than 161 million visually impaired people. Thirty-seven million people were blind and one-hundred twenty four million people had low vision. Low vision interferes with many daily activities. It affects a person's academic and economic life and even his/her social life. Patients with low vision have many different goals for their low vision rehabilitation. Reading is one of the most common goals reported by adults with low vision.2 Unlike adults with low vision, low vision may cause a lifelong reduction in a child's visual performance.3 Reading is one of the main avenues for education and educational achievement. If visual impairment affects the child's ability to read, it could be a great impediment of his/her educational success.4 Read ing is a first step in education and is a predictor of good aca demic success.5 The first barrier to reading for most children with low vision is the print size. Children with low vision usually need some form of magnification to resolve letters that are lower than their threshold.6 During a low vision assessment, reading performance is not assessed expect for a brief assessment of thresholds and fluency.7 With a detailed low vision examination and an accurate visual correction, children might achieve a better reading performance. There are other examinations than visual acuity that should be included in the low vision examina tion. Acuity reserve and contrast reserve are good predic tors of reading performance in adults and are likely to be important in children. The optimum magnification, acuity reserve and contrast reserve tend to lead to the optimum possible reading fluency.
In this paper we review the literature that relates to visual reading in children with low vision with an emphasis on visual requirements in terms of acuity (or magnification), contrast and visual field.
Relationship to visual acuityA typical low vision examination always includes a visual acuity test. Visual acuity on its own used to be considered as the only predictor of reading ability.8 Recent studies have shown that this is not the whole story.8,9 Whittaker and Lovie-Kitchin 8 defined the Acuity Reserve as the ratio of the print size of the reading material to the subject's visual acuity threshold for a particular print being read. With a 1:1 acuity reserve, i.e., or no acuity reserve patients can still read, but very slowly. With the optimum acuity reserve patients can read more easily and have a higher reading rate. Whittaker and Lovie-Kitchin used published data from three previous studies 10-12 and re-plotted the results to show the effect of acuity reserve on reading speed. Also, they indicated that the majority of low vision professionals tend to work with patients who, at the time of assessment, had an acuity reserve of 3:1 or less. An acuity reserve of 18:1 was the maximum of the optimum acuity reserve range and with higher reserves than this, the reading rate drops. For most adults an acuity reserve between 6:1 and 18:1 is required to achieve maximum reading rate.8
Kestenbaum and Sturman 13 suggested a rule to calculate the reading addition for a given visual acuity. Kestenbaum's rule is that the reading addition equals the inverse of the visual acuity. It tends tounder estimate the reading addition for a patient 14 and results in the person reading close to the resolution limit. Kestenbaum's rule is mainly used as a starting point for the required reading addition. Most derivatives from Kestenbaum's rule reported an additional magnification factor to the original rule of 1.5 to 2.0×.14 Clinically, professionals suggested more magnification or acuity reserve for better reading performance.14 Raasch and Rubin, in a study of patients with age-related macular degeneration, argued that patients need 6× or maybe more than Kesten baum's rule to achieve the maximum reading rate.14
In a study on sighted children by Lueck et al., 15 a comparison was made of the required visual acuity reserve for reading text and unrelated words. The results indicated that four times acuity reserve is needed for sighted children to read text materials aloud. Less acuity reserve is required to read unrelated words.
A more recent study of Lueck et al.16 showed that children with low vision need at least three times the acuity reserve to read efficiently. This results in much larger print sizes being required for children with very low visual acuities in order for them to gain the optimum acuity reserve. Lueck et al. 16 reviewed some ways that help children with low vision achieve the optimum acuity reserve. These include decreasing the reading distance, increasing the print size material or using a low vision aid.
Lovie-Kitchin et al. 17 reported a study of adults and children with low vision that showed that the acuity reserve for children should be between 2.5:1 and 8:1 and between 2:1 and 8:1 for adults for maximum reading rates to be achieved. These results are lower than Whittaker and Lovie-Kitchin 8 found for adults but there is some overlap.
In another study on children by Lovie-Kitchin et al., 4 acuity reserve between 2.5:1 to 7:1 was necessary to achieve maximum reading rate. Patients with lower visual acuities tend to achieve maximum reading rate with less acuity reserve, which was an unexpected result in this particular study and in contrast to Lueck et al. above. 16 Interestingly they found that, unlike adults with low vision, age was a better predictor of reading rate than near visual acuity in children with low vision.
A variety of reading tests have been used for these studies. Some studies have used standardised tests of reading and some researchers have developed their own tests of reading based on similar principles. Figure 1 and 2 show examples of reading cards that have been used. Lueck et al. 15,16 used the Bailey-Lovie Word reading cards and sentences from the MNRead test (Figure 2) while Lovie-Kitchin et al. 17 used the Bailey-Lovie Word reading cards and charts created from standardised children's texts.


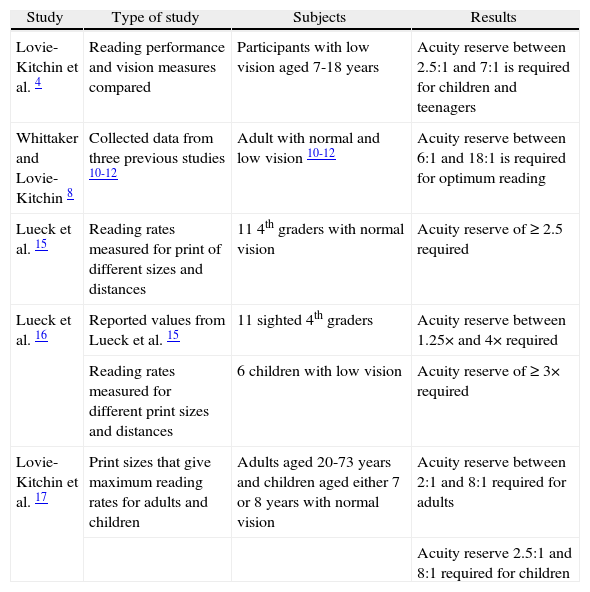
Thus, there are only three studies on how much acuity reserve is needed for children to achieve maximum reading rate. It ranged between 2.5:1 and 8:1. Further studies for children should be done to confirm these results. Table 1 summarises the results of studies that measured acuity reserves in adults or children.
Studies of acuity reserve
| Study | Type of study | Subjects | Results |
| Lovie-Kitchin et al. 4 | Reading performance and vision measures compared | Participants with low vision aged 7-18 years | Acuity reserve between 2.5:1 and 7:1 is required for children and teenagers |
| Whittaker and Lovie-Kitchin 8 | Collected data from three previous studies 10-12 | Adult with normal and low vision 10-12 | Acuity reserve between 6:1 and 18:1 is required for optimum reading |
| Lueck et al. 15 | Reading rates measured for print of different sizes and distances | 11 4th graders with normal vision | Acuity reserve of ≥ 2.5 required |
| Lueck et al. 16 | Reported values from Lueck et al. 15 | 11 sighted 4th graders | Acuity reserve between 1.25× and 4× required |
| Reading rates measured for different print sizes and distances | 6 children with low vision | Acuity reserve of ≥ 3× required | |
| Lovie-Kitchin et al. 17 | Print sizes that give maximum reading rates for adults and children | Adults aged 20-73 years and children aged either 7 or 8 years with normal vision | Acuity reserve between 2:1 and 8:1 required for adults |
| Acuity reserve 2.5:1 and 8:1 required for children |
The first common impediment of reading for low vision patients is the text print size. Different methods can be used to magnify text and give better reading performance. In the literature on this subject, eye care professionals and educators have debated whether it is more beneficial to use a magnifier or large print text to obtain magnification. According to McCurry et al., 18 most children with low vision tend to benefit from using magnifiers to read standard print. In this study, all of the children underwent a regular low vision assessment of their visual performance. This included a reading performance evaluation using a magnifier. The study's aim was to determine the effectiveness of using magnifiers to read standard print size. The results showed that near vision performance was improved for 28% of the children with spectacles and/or magnifiers and that 54.3% of the children were enabled to read standard print size. Also, nearly half of the children showed improvement in their reading and/or writing skills with spectacles and/or magnifiers. In addition, the study reported that most magnifiers used were stand magnifiers. This study is in agreement with Leat and Karadsheh's 19 study, in which it was reported that stand magnifiers tend to be the first choice of near low vision aids by children.
Farmer and Morse's study 20 made a comparison between two groups of children. The first group of children used large-print text for reading while the second group used magnifiers. The results showed that the first group had an increase in reading speed rates but with no significant increase in reading comprehension skills. On the other hand, the second group of children showed an increase in their reading speed rates and a noticeable increase in their reading comprehension skills.
In a study by Kalloniatis and Johnston7, children's clinic files were reviewed to find relevant data. Then the children's reading performance was assessed in their regular classroom with the use of their low vision aids. In general, the children had a high rate of low vision aids usage. More specifically, it was also found that the children's vision could be improved by using simple low vision aids. The study concluded that the children preferred to move their reading material closer (use a close reading distance) than to use a low-powered near low vision aid.
In the study by Silver et al.,21 which included 230 children at a school for the blind, visual acuity was used to determine the need for magnification or glasses. The majority of these children (57%) were only taught Braille and treated as totally blind, although 79% of these children could benefit from near low vision devices or reading spectacles and be enabled to read normal print. This study raises the importance of magnification, and the effect on the children's academic life. This study also reported that stand magnifiers seem to be the easiest optical magnifiers for children to use.
Thus there is only one study that directly compares optical magnification with large print and this showed that using magnifiers was more effective compared to providing large print text. Many studies, however, have described the benefits of optical magnification3,18,20,21 to help children with visual impairment to read. Using magnifiers does not limit the childrens’ reading material to that which is enlarged only and allows children to access any written information in normal print size. Producing large print books is expensive. However, enlarging photocopying is more available nowadays and also changing the font size on a computer document is easy. Magnifiers are also the only option for children who require higher levels of magnification for whom providing large print materials is impossible, although a combination of large print and optical magnification is also an option. Thus it seems that, for better education achievement, children with low vision should be assessed for magnifiers and be taught and trained how to use them effectively.
Relationship to contrast reserveAccording to Whittaker and Lovie-Kitchin,8 the ratio of the letter contrast to the subject's contrast threshold for a reading print is defined as the Contrast Reverse. Decreased print contrast and also decreased contrast sensitivity of the observer results in a reduction of the contrast reserve. In this study of adults with low vision, Whittaker and Lovie-Kitchin used published data from three different experiments.9,22,23 Results were re-plotted together and it was found that decreasing contrast reserve resulted in declined reading rate. People with normal sight also experience low reading rates if the contrast reserve is less than 20:1 8. Whittaker and Lovie-Kitchin8 suggested that the optimum contrast reserve for maximum reading rate is higher than 30:1 and for high fluent reading a reserve of 10:1 is required. Also, it was found that for 6 degree letters the majority of patients with low vision have a 0.10 or higher contrast threshold.9 Thus patients with low vision have reduced reading rate because, even with video magnifiers that give a contrast of almost 1 (100%) and plenty of magnification, their contrast reserve may be less than 10:1.8
In a study of young normally sighted adults, Mohammed and Dickinson, 24 studied the effect of contrast reserve on reading performance. This was evaluated by comparing different magnification powers with controlled field of view. It was found that providing the patient with higher magnification could not compensate for a low contrast reserve and thus lead to a more optimum reading rate. It was found that reading performance declined whatever the level of magnification if the contrast reserve was lower than 10.5:1, which is in agreement with the study by Whittaker and Lovie-Kitchin.8
According to Leat and Woodhouse, 25 contrast sensitivity was a predictor of reading speed. The study included 30 adult subjects. The authors concluded that contrast sensitivity at 0.5 c/deg was correlated with reading performance and contrast sensitivity at high spatial frequencies was a poorer predictor of reading speed compared to contrast sensitivity at the lower spatial frequencies. The study suggested that contrast sensitivity should be included in a regular low vision assessment.
A recent study by Lovie-Kitchin et al.,4 the only study of contrast sensitivity and reading in children, found quite different results than those reported in adults with low vision.8,24,25 In this study, the contrast sensitivity for 71 students (aged 7-18 years) was measured at low to mid spatial frequencies. However, it must be noted that the children generally had relatively good contrast sensitivity. Only four children had contrast sensitivity less than 10. It was concluded that, unlike adults with low vision, contrast sensitivity was not a good predictor of reading rate in children with low vision and it would not be helpful to include a contrast sensitivity measurement routinely in a clinical low vision assessment for reading in this population.
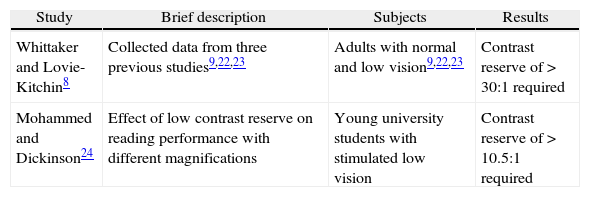
Table 2 summarises the results of studies that measured contrast reserves in adults or children.
Studies of contrast reserve
| Study | Brief description | Subjects | Results |
| Whittaker and Lovie-Kitchin8 | Collected data from three previous studies9,22,23 | Adults with normal and low vision9,22,23 | Contrast reserve of > 30:1 required |
| Mohammed and Dickinson24 | Effect of low contrast reserve on reading performance with different magnifications | Young university students with stimulated low vision | Contrast reserve of > 10.5:1 required |
In the study by Whittaker and Lovie-Kitchin,8 the results of two studies 12,26 of adult subjects with normal and low vision were re-plotted. It was found that, for both normal and low vision subjects, reading rate increased as field of view increased. Subjects with low vision use low vision devices and usually need to move the reading material as close as possible to the eye.8 The authors suggested that the field of view restricted by simple low vision devices is not significant. It was also concluded that, if people with low vision are taught to manipulate the low vision device and place the text within the field of view of the device, a large field of view is not necessary for fast reading rate.
In a study by Legge et al.,27 141 adults with low vision were included. The study's aim was to determine which clinical measurement was a good predictor of reading speed. Field of view was examined by Goldmann perimeter or tangent screen. If the subject had a scotoma that covered all or part of the central 5° of the visual field he/she was classified as having central loss. If not, he/she was classified as having central field intact. It was found that central visual field loss was associated with slow reading speed. It was, however, not a predictor of slow reading speed. On the other hand, it was found that the majority (74%) of slow readers had central loss.
According to Gompel et al.,28 visual field defects do not affect children's reading speed and comprehension. This study compared two groups of children with low vision. The first group included children with low vision who had visual field restrictions and the second group were children with low vision and intact visual fields. Interestingly, no differences in reading speed and reading-comprehension skills were found between these two groups of children with low vision. This is the only study on the effect of visual field constrictions on reading speed rate in children with low vision. More studies need to investigate the importance of field of view on reading speed in children with low vision.
ConclusionAdults with low vision can read effectively when the main criteria for good reading are met. These include magnification, acuity reserve, contrast reserve and visual field. Little is known about the similar requirements for children. It does appear that acuity reserve should be at least 2.5:1.4,17 This can be achieved by increasing the magnification which may possibly help to compensate for any low contrast reserve. There have been no studies that have investigated the minimum contrast reserve required for children with low vision to read easily, although one study showed that contrast sensitivity may be less of a limitation in young people than older adults. In adults, a contrast reserve of more than 10:1 8,24 is needed to achieve the optimum reading speed rate. Using electronic magnifiers or high contrast print could help to compensate for low contrast sensitivity for the children with low vision and good illumination may improve contrast sensitivity in some cases. Children with clear media and intact central visual field should be able to read reasonably well. Adequate magnification resulting in a good acuity reserve and contrast reserve would be expected to lead to better reading performance.
Thus there are indications that children do not perform in exactly the same way as adults4 and the adult data may not be directly applicable to children. Further studies for children should be done to further investigate the parameters that may affect childrens’ reading performance so as to further our knowledge and improve the clinical assessment of reading and provision of reading aids in children.
Conflict of interestThe authors state they have no conflict of interest.





