


Patterns of refractive errors have never been reported in Maldives. This study aims to dissect astigmatism and provide a general view in context of this island country.
MethodsA clinic based cross sectional study was designed with 277 patients, aged ≥3.5 years and with a primary astigmatism of ≥−1.00 diopters (D). They underwent complete eye examination and a vector analysis was done.
ResultsMean age was 28.58 (SD 19.15) years. Astigmatic magnitude depended on age (p<0.05) but not on gender (p>0.05). Severity of visual impairment after refractive correction was very less, with only 2.2% having visual acuity ≤6/60. Mean spherical, spherical equivalent and astigmatic refraction were −1.35 (SD 2.94D), −2.40 (SD 3.04) and −2.12 (SD 1.11D), respectively. Between fellow eyes, refractive and corneal astigmatism highly correlated (0.83 and 0.73). Fifty eyes (18.1%) had an astigmatic error of ≥−3.00D which peaked in the second and third decades of life (p<0.0001) and was corneal in origin (p<0.0001). Internal J45 and J0 tended to be more negative with increasing age, showing a trend toward against the rule astigmatism. Correlation between corneal and refractive J0 and J45 were 0.88 and 0.62 (p<0.0001). With the rule astigmatism was more common followed by against the rule and oblique.
ConclusionIn conclusion, this study inferred that among patients with relatively higher magnitude of astigmatism attending to the clinics in Maldives, younger patients are affected more, which could possibly link to the environment, genetics and nutrition. The probable association between nutrition and astigmatism needs to be investigated to fill the gap in literature.
Los patrones de los errores refractivos no han sido reportados nunca en Maldivas. Este estudio trata de analizar minuciosamente el astigmatismo, así como aportar una visión genérica en el contexto de este país insular.
MétodosSe diseñó un estudio clínico transversal que incluyó a 277 pacientes, de edades ≥3,5 años y con astigmatismo primario de ≥-1,00 Dioptrías (D). Se les realizó un examen visual completo y un análisis vectorial.
ResultadosLa edad media fue de 28,58 años (DE 19,15). La magnitud astigmática dependió de la edad (p<0,05) pero no del sexo (p>0,05). La severidad de la discapacidad visual tras la corrección refractiva fue muy baja, y únicamente el 2.2% reflejó una agudeza visual ≤6/60. La media del defecto esférico, el equivalente esférico y la refracción astigmática fueron de -1,35 (DE 2,94D), -2,40 (DE 3,04) y -2,12 (DE 1,11D), respectivamente. El astigmatismo refractivo y el corneal guardaron una amplia correlación entre ambos ojos (0,83 y 0,73). Cincuenta sujetos (18,1%) reflejaron un valor de error astigmático ≥-3,00D, que se incrementó en la veintena y la treintena (p<0,0001), siendo corneal en origen (p<0,0001). Los vectores J45 y J0 internos tendieron a ser más negativos conforme aumentaba la edad, mostrando tendencias de astigmatismo en contra de la regla. La correlación entre los vectores J0 y J45 corneal y refractivo fue de 0,88 y 0,62 (p<0,0001). El astigmatismo a favor de la regla fue el más común, seguido del astigmatismo contra la regla y el oblicuo.
ConclusiónEn conclusión, este estudio concluyó que de entre los pacientes astigmáticos de magnitud relativamente mayor que se presentaron en la clínica de Maldivas, los pacientes más jóvenes estaban más afectados, lo que podría estar ligado al entorno, los factores genéticos y la nutrición. Debe investigarse la posible asociación entre la alimentación y el astigmatismo, para llenar el vacío en la literatura al respecto.
Astigmatism is a clinically important condition and accounts for about 13% of the refractive errors of human eye.1 Its prevalence (≤0.50D) has been reported to vary with ethnicity,2 age,3 and sex.2 In the Sydney Myopia Study, 4.8% of 6-year-old children had refractive astigmatism (≤−1.00D)4 which was similar to that reported in Finland (3.8%)5 and Southern urban and rural India (3.8%)6,7 as well as in Poland (4%).8 The prevalence of refractive astigmatism in Australian children is much lower than that in Chinese (38.6%)9 Taiwanese (14.6%)10 and Singaporean children (19.2%).11 This regional and ethnic variation is also found in adult populations.12
Astigmatism influences the normal visual development13 and may cause amblyopia in children.14 Presence of early astigmatism relates to the development of myopia, possibly through the signal driven by astigmatic blur which either aids or disrupts the emmetropization of the spherical power.15 It is found that most astigmatic corneas occur in newborns with the lowest birth weight and lowest post-conceptional age16 Likewise, infants have large degrees of astigmatism which decline through emmetropization17 and may remain in a small degree (≤−1.00D) by the age of four years.18 In a longitudinal study, Gwaizda et al. indicated that 4–5 years is a time of transition for astigmatism as it changes from Against-The-Rule (ATR) to With-The-Rule (WTR). If a child does not have astigmatism in infancy, he or she is unlikely to acquire it at a later age, at least up to 4–6 years of age.19
Family studies have supported the role of genetics in astigmatism.12 Clementi and colleagues defined the genetic model for corneal astigmatism and provided an evidence for Single Major Locus (SML; a multifactorial transmissible component) inheritance.20 The genes in myopia twin study (GEM) supported a strong genetic component in astigmatism21 which demonstrated a genetic component to corneal curvature. Valluri and colleagues reported a stronger role for environmental factors.22
The trends of refractive errors and other ocular diseases are unknown in Maldives which is an island country of Islamic religion. Most of the patients here present to the clinic with relatively higher magnitude of astigmatism. This study was designed to investigate astigmatism in relation to age and gender, and it is expected that the reports of present study form the baseline evidence for further cohort studies to explain the possible etiology of the high magnitude astigmatism in this island country.
Methods and methodologyThis is a cross sectional, descriptive study carried out in Eye Care Hospital, Maldives. Patients satisfying the inclusion criteria were included randomly over a period of 3 months since July 2013. The tenets of the declaration of Helsinki were adhered to and the informed consent was taken either from the parents (for young subjects) or patients themselves. The inclusion criteria were set as follows: age ≥3.5 years (emmetropization completes by this age), physical and mental wellbeing, able to cooperate adequately for the complete ocular examination including refraction and keratometry, and astigmatism ≥−1.00D. Astigmatism ≥−1.00D was set as cut off value because usually this is considered as clinically significant and it will facilitate the comparison of magnitude with other factors. Patients with foreign origin other than Maldives, with corneal scars and/or diseases, with obvious syndromes and other conditions which could affect corneal topography and with history of past ocular surgery were excluded. All the patients were first examined by an ophthalmologist before being sent for consultation with an optometrist who enrolled the patients in the study subject to check if they meet the inclusion criteria. Care was taken not to include the patients with ocular pathology that could interfere with the visual improvement after appropriate refractive correction.
A complete eye examination was done which included: Visual Acuity (VA) testing (unaided and aided, tested with mirror chart), keratometry and objective refraction (Topcon KR 8800), subjective refraction (Phoropter, Topcon CV 3000), retinoscopy when indicated, slit lamp examination and funduscopy. Cyclorefraction was done in very young children, unmatched objective and subjective refraction, fluctuating errors, fluctuating fixation, VA not corresponding to refractive errors, patients not cooperating in the examinations, and in oculomotor imbalances. To compare the accuracy of the autorefractors, three optometrists (SM, SU and JB) performed objective refractions among each other to check for repeatability. This is the part of the regular verification process carried out in the clinic to ensure the accuracy of the instrument. It was observed that spherical components varied between ±0.25 to ±0.50 and the repeated measurements ensured minimum difference or no difference whereas the cylindrical components were exact in all the observations. Three optometrists have different degrees of refractive errors (SU; −0.75 DS in both eyes, JB; −1.50/−1.50×90 in right eye and −1.50/−1.50×80 in left eye and SM; −0.25DS both eyes). For the purpose of data analysis, objective refraction was taken into account.
Autorefractor findings (for both corneal curvatures and objective refractions) were recorded as an average of minimum five measurements which ensured the minimal errors. Autorefractometer uses corneal refractive index of 1.3375 to compute the corneal powers. Corneal astigmatism was calculated based on auto-keratometric reading as the difference between the maximum and minimum corneal power, with the cylinder axis set at the corneal meridian with minimum power. All refractions were noted in minus cylinder convention. Astigmatism was classified as WTR if the minus cylinder axis was at 180°±15°, ATR for minus cylinder at 90°±15°, or oblique (other than WTR or ATR). 23 For each measurements, the refractive and corneal astigmatism were converted from their sphero-cylinder notation to vector notation using the following equations:24


where ‘C’ is cylinder and ‘a’ is cylinder axis. In this representation, positive and negative values of J0 indicate WTR and ATR astigmatism, respectively, whereas J45 accounts for the oblique component of the astigmatism. Otherwise indicated, right eye was selected for analysis. We selected only the right eye because the findings in both the eyes of same individual are generally likely to be similar.25
All the ocular findings were entered in the Optical software TOLPIT (Linoptica SA). The use of this software minimized the risks of case repetition. TOLPIT records all the patient information including ID number, age, gender, address, previous history of diseases/surgeries, mode of refractive correction (glasses, spectacles), number of months/years since the first use of refractive correction, clinical profile, visual acuity notations, refraction procedures, clinical impression and the treatment advised.
StatisticsStatistical analysis was performed using the statistical software package SPSS 19.0 for Windows. The correlation of different components of astigmatism between two eyes were tested with Pearson correlation coefficients (bivariate) and categorical data were analyzed with Chi-Square test (astigmatic magnitude against gender and age category).
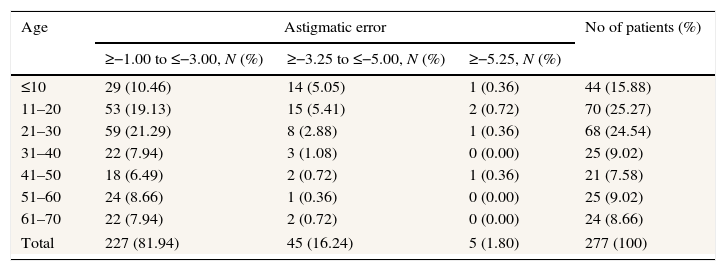
ResultsCharacteristics of the study populationOf 326 eligible patients, 34 were not included in the analysis either because of lack of parental consent (16) or self-denial (18). Nine patients were excluded from the analysis as their data was missing either on keratometry, autorefraction or visual acuity. Six children were excluded either because they did not stay still for keratometry or refraction could not be done accurately. Among 277 patients included, 153 (55.2%) were male. Mean age was 28.58 (SD 19.15) years {range 3.5–67 years with 41% (114) up to 20 years and 66% (182) up to 30 years}(Table 1). Table 1 shows that most of the astigmatic errors were within −3.00 diopters (82%) and age below 30 (66%).
Distribution of age and astigmatism.
| Age | Astigmatic error | No of patients (%) | ||
|---|---|---|---|---|
| ≥−1.00 to ≤−3.00, N (%) | ≥−3.25 to ≤−5.00, N (%) | ≥−5.25, N (%) | ||
| ≤10 | 29 (10.46) | 14 (5.05) | 1 (0.36) | 44 (15.88) |
| 11–20 | 53 (19.13) | 15 (5.41) | 2 (0.72) | 70 (25.27) |
| 21–30 | 59 (21.29) | 8 (2.88) | 1 (0.36) | 68 (24.54) |
| 31–40 | 22 (7.94) | 3 (1.08) | 0 (0.00) | 25 (9.02) |
| 41–50 | 18 (6.49) | 2 (0.72) | 1 (0.36) | 21 (7.58) |
| 51–60 | 24 (8.66) | 1 (0.36) | 0 (0.00) | 25 (9.02) |
| 61–70 | 22 (7.94) | 2 (0.72) | 0 (0.00) | 24 (8.66) |
| Total | 227 (81.94) | 45 (16.24) | 5 (1.80) | 277 (100) |
Many patients (38%, 105) had presenting visual acuity normal (Snellen Chart 6/6) to subnormal (Snellen chart ≤6/12) and only 40 (14.5%) had visual acuity of less than or equivalent to 6/60. After the refractive correction, only 6(2.2%) had visual acuity less than 6/60 (Fig. 1).
Distribution of the magnitude of astigmatism
Mean spherical and astigmatic refractive errors were −1.35(SD 2.94 D) and −2.12 (SD 1.11D), respectively. Pearson correlations between right and left eye refractive astigmatism (RA) and corneal astigmatism (CA) were 0.83 (P<0.0001) and 0.73 (P<0.0001), respectively, and the difference between eyes for RA and CA were 0.03 (SD 1.59) and 0.04 (SD 1.49). Majority of the patients (81.9%, 227) had total astigmatic component ≥−3.00D.
Variations with ageAstigmatic magnitude was dependent on age (Chi Square test, p<0.001) and astigmatic value ≥−3.00D was more common in age group below 20 (Chi Square test, p<0.001) (Table 1). Mainly young patients (age below 20 years) had corneal astigmatism (Chi Square test, p<0.0001) and it decreased with age.
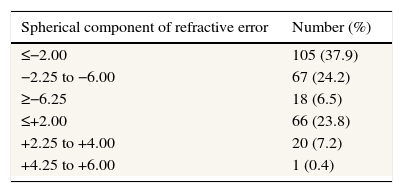
Distribution of spherical errorMean spherical equivalent refractive error was −2.40 (SD 3.04) and myopia was more common (68.6%) (Table 2). Out of 190 myopic patients, 91 (26.4%) were below 20 years and out of 87 hyperopic subjects, 23 (47.9%) were below 20 years.
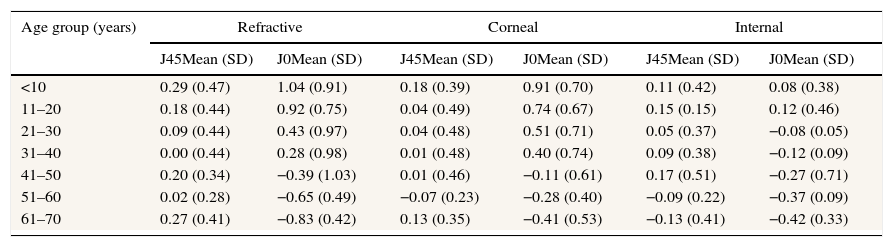
Variations in mean astigmatismMean values for refractive, corneal and internal J45 and J0 were 0.15 (SD 0.43), 0.04 (SD 0.43), 0.10 (SD 0.37) and 0.36 (SD 1.05), 0.44 (SD 0.79) and −0.07 (SD 0.49) diopters, respectively. Internal J45 and J0 tended to be more negative with increasing age, showing a trend toward against the rule astigmatism (Table 3).
Astigmatic components categorized with age groups.
| Age group (years) | Refractive | Corneal | Internal | |||
|---|---|---|---|---|---|---|
| J45Mean (SD) | J0Mean (SD) | J45Mean (SD) | J0Mean (SD) | J45Mean (SD) | J0Mean (SD) | |
| <10 | 0.29 (0.47) | 1.04 (0.91) | 0.18 (0.39) | 0.91 (0.70) | 0.11 (0.42) | 0.08 (0.38) |
| 11–20 | 0.18 (0.44) | 0.92 (0.75) | 0.04 (0.49) | 0.74 (0.67) | 0.15 (0.15) | 0.12 (0.46) |
| 21–30 | 0.09 (0.44) | 0.43 (0.97) | 0.04 (0.48) | 0.51 (0.71) | 0.05 (0.37) | −0.08 (0.05) |
| 31–40 | 0.00 (0.44) | 0.28 (0.98) | 0.01 (0.48) | 0.40 (0.74) | 0.09 (0.38) | −0.12 (0.09) |
| 41–50 | 0.20 (0.34) | −0.39 (1.03) | 0.01 (0.46) | −0.11 (0.61) | 0.17 (0.51) | −0.27 (0.71) |
| 51–60 | 0.02 (0.28) | −0.65 (0.49) | −0.07 (0.23) | −0.28 (0.40) | −0.09 (0.22) | −0.37 (0.09) |
| 61–70 | 0.27 (0.41) | −0.83 (0.42) | 0.13 (0.35) | −0.41 (0.53) | −0.13 (0.41) | −0.42 (0.33) |
Values for refractive J45 were higher than for corneal J45 and there was a significant correlation between them (Bivariate Pearson Correlation, two tailed, r=0.62, p<0.001) (Table 3). On scatter plot between refractive and corneal J0, most of the values were below the line of unit slope, indicating that most of the patients had more corneal astigmatism than refractive astigmatism along the Cartesian axis (Fig. 2). Corneal and refractive J0 and J45 did not differ statistically (Bivariate Pearson Correlation, two tailed, r=1.11, p>0.05).
Variations in the axis of astigmatism
With the rule astigmatism (WTR) was more common followed by ATR and oblique (48.7%, and 30.3% and 20.9%, respectively). Below 10 years, WTR was common and beyond 40 ATR was common. Oblique astigmatism had no definite trend, but was more common in 21–30 (18/68) and in >41 years (18/70). Astigmatic magnitude was independent of gender (P>0.05).
DiscussionThis study is the first refractive error study in Maldives. Results show that astigmatic magnitude changes gradually with age but is independent of gender. Most of the astigmatic errors are within −3.00D and very common in school going children. This observation is in contrast to the data from Dobson and colleagues26 and Gwaizda et al.19 who report that large astigmatic errors seen during infancy are eliminated or reduced greatly by school age. We noted simple astigmatism as high as −9.00D. The prevalence of such high degree astigmatism may be correlated to genetics, environment and nutritional factors.
Ethnic variation of astigmatism has been extensively studied previously. Higher prevalence (≥1.00D) has been reported in Native American school children (42%),27 East Asian subjects and Chinese school children.28 It has been postulated that these high degrees of WTR astigmatism probably relate to heredity or nutritional factors. Poor nutrition may lead to reduced corneal rigidity which results in increased corneal astigmatism due to pressure from the upper eyelid that flattens cornea in the horizontal meridian and makes steeper the vertical.29 Moreover, the greater tightness of the Asian eyelids and narrower palpebral apertures may have some role.28 The common Maldivian dishes are sea foods which are rich sources of Omega-3 fatty acids. The nutritional benefits of omega-3-fatty acids to the human being has been studied extensively and are found effective in relieving dry eye symptoms,30 enhancing infant vision development,31 and possibly in preventing macular diseases.32 A recent medical study on rat muscle fibers shows that diets rich in Omega-3 and Omega-6 fatty acids produce 16–21 percent more muscle tension and have up to 32 percent greater endurance during high frequency stimulation33 which shows a possibility that Maldivians have higher lid tonicity which could link to the regular intake of sea foods. Although, it seems rather speculative to hypothesize above statement, a carefully designed cohort study can assess the association between lid and corneal structural and physiological changes with nutritional status. It will provide an insight on the astigmatic origin in this Islamic island country. The current literature search could not associate nutrition with astigmatism but the role of nutrition on the development of myopia has been studied previously.34
In our study, refractive and corneal astigmatic errors were similar, a comparable finding as seen in Northen Ireland in school going children with similar definitions.35 Although, age category of our subjects ranged from very young to old, the axis distribution is similar to the reports of Gwaizda et al. who reported ATR in very young children and WTR in later stages.19 Literature anonymously supports the role of increased eye lid pressure in variation of astigmatic axis in young population.28,29 We observed that WTR astigmatism was more common followed by ATR and oblique (48.7%, 30.3% and 20.9%, respectively). Although the frequency differed (11.7%, 18.1%, and 2.4%), the variation in the axes is similar to that of a population based study in Iran.36 The difference in the frequency could be because of the sample size difference.
Severity of the visual impairment was very less with only 14.5% having presenting visual acuity 6/60 or less which improved significantly after refraction. As very few patients had hyperopic astigmatism, only few of them could not achieve significant visual acuity improvement because of meridional amblyopia. We did not find statistically significant difference between sex and magnitude of astigmatism, an observation similar to that of Fotouhi et al. in Iran.37
This study attempted to dissect astigmatism in Maldives and showed that high magnitude astigmatism present frequently in the clinics. The study patients were selected carefully to facilitate the comparison of astigmatic magnitude with various factors. Because of the aim and scope of the study, it has retained some limitations. First, patients were selected from a clinic that came seeking an advice, so it may not provide the true picture of astigmatic status in the country; second, sample size was relatively small to generalize the findings and; third, we ignored low magnitude astigmatism. However, as this is the first study done in refractive errors in this island country, and the variation in astigmatism seems to differ from other parts of the world, it is expected that this study will trigger further prospective cohort studies to investigate astigmatism in relation to nutrition. It will fill the gap in the literature and will help to improve the visual status of Maldivians.
In conclusion, this study inferred that from patients with relatively higher magnitude astigmatism attending to the clinics in Maldives, younger patients were affected more, which could possibly link to the environment, genetics and nutrition. The probable association between nutrition and astigmatism needs to be investigated in cohort studies to fill the gap in literature.
I would like to thank Eye Care Hospital Pvt Ltd. for providing me consent to conduct this study with an adequate access to TOLPIT software. I sincerely thank my optometry colleagues Mr Jeewanand Bist; BOptom (JB) and Dr Santosh Upadhyaya; BOptom, OD (SU) and Dr Srinivas Shetty (MD, Ophth) for their advices and in patient co-management.


www.publicationethics.org.



