

To test the hypothesis that human eyes have a central tendency to be free of higher-order aberrations by analyzing wavefront aberrations for two young populations of respectively emmetropic and myopic subjects.
MethodsBoth right and left eyes of 75 emmetropes and 196 myopes were measured for corneal wavefront aberration using a Humphrey corneal topographer and for the whole eye wavefront aberration using a WASCA wavefront sensor without pupil dilation. 35 Zernike aberration coefficients over a 6.0mm pupil diameter were derived, and statistics of the higher-order terms (3rd to 5th orders) were tested.
ResultsWhen signed Zernike aberrations of the right and left eyes were averaged together for the emmetropes, three higher-order modes (j=6, 12 and 13) were significantly different from zero in both the cornea and the whole eye (P<0.0005), and three additional terms (j=14, 15 and 17) were statistically non-zero for the whole eye. As the signs of y-axis asymmetrical terms in the left eye were flipped, three more terms in either the cornea (j=8, 18 and 19) or the whole eye (j=8, 10 and 20) became statistically non-zero. For the myopes, 8 corneal terms and 5 whole-eye terms were statistically non-zero when the two eyes were averaged together. As the signs flipped, the majority of the Zernike aberration terms were statistically different from zero.
ConclusionsHuman eyes have systematical higher order aberrations in population, and factors that cause bilateral symmetry of wavefront aberrations between the right and left eyes made important contribution to the systematical aberrations.
Poner a prueba la hipótesis de que el ojo humano, en promedio, tiende a estar libre de aberraciones de alto orden. Para ello se analizó la aberración de onda en dos poblaciones distintas: una compuesta por jóvenes emétropes, la otra por jóvenes miopes.
MétodosSe estudiaron los ojos izquierdo y derecho de 75 emétropes y de 196 miopes. En cada ojo, sin dilatar la pupila, se midieron las aberraciones corneales utilizando un topógrafo corneal Humprey y también se obtuvo la aberración de onda de toda la óptica ocular por medio de un sensor de frente de onda WASCA. A partir de estos datos se calcularon los 35 coeficientes de aberración de Zernike que caracterizan cada patrón de aberración para un diámetro de pupila de 6,00mm, realizándose a continuación un análisis estadístico de los términos de alto orden (del 3° al 5° orden).
ResultadosCuando para los emétropes se promedian los coeficientes de aberración de Zernike para los ojos izquierdo y derecho, manteniendo su signo, hay tres modos de alto orden (j=6, 12 y 13) que resultan ser significativamente distintos de cero, tanto para la córnea como para todo el ojo. Además, otros tres términos (j=14, 15 y 17) resultaron ser también estadísticamente distintos de cero cuando se analiza todo el ojo en su conjunto. Cuando se cambia para el ojo izquierdo el signo de los coeficientes correspondientes a los términos de aberración que son asimétricos respecto al eje y, hay tres términos más (en la córnea: j=8, 18 y 19, y para todo el ojo: j=8, 10 y 20) que pasan a ser estadísticamente distintos de cero. En lo que respecta a los miopes, hay 8 términos para la córnea y 5 términos para todo el ojo que resultan ser estadísticamente distintos de cero cuando se promedian los dos ojos de todos los integrantes del grupo. Cuando se cambian los signos, de forma análoga al grupo anterior, la mayoría de los coeficientes de aberración de Zernike resultan ser estadísticamente distintos de cero.
ConclusionesEl ojo humano presenta de forma sistemática aberraciones de alto orden. Los factores que provocan la simetría bilateral de la aberración de onda entre el ojo izquierdo y derecho de cada individuo contribuyen de manera importante a la presencia de dichas aberraciones sistemáticas.
Recent improvements in aberrometry have made a fast and precise measurement of wavefront aberrations in the human eye possible not only in the laboratory for eye research but also in the offices of optometry and ophthalmology for clinical diagnosis. Consequently, a number of studies have been conducted to investigate the nature of wavefront aberrations in the human eye (e.g. see reviews by Applegate,1 Thibos,2 and Charman3). For the normal population, the human eye has been believed to have a central tendency to be free of higher-order aberrations, because the mean of the higher-order Zernike modes, excluding the spherical aberration,3-4 for each individual Zernike term, were not significantly different from zero, even though none of the higher-order aberrations for a single eye was by any means equal to zero. Results supporting the hypothesis of the population being free of higher-order aberrations arose mainly from three population studies that used experimental systems constructed in the laboratory.4-6 If the hypothesis was true, it could imply, from the viewpoint of eye research, that the eye is very well corrected of its higher-order aberrations under the pressure of nature selection, despite the existence of substantial individual variation. Meanwhile, from the viewpoint of clinical practice, the optimal goal for eye treatment is to correct the higher-order aberrations completely.
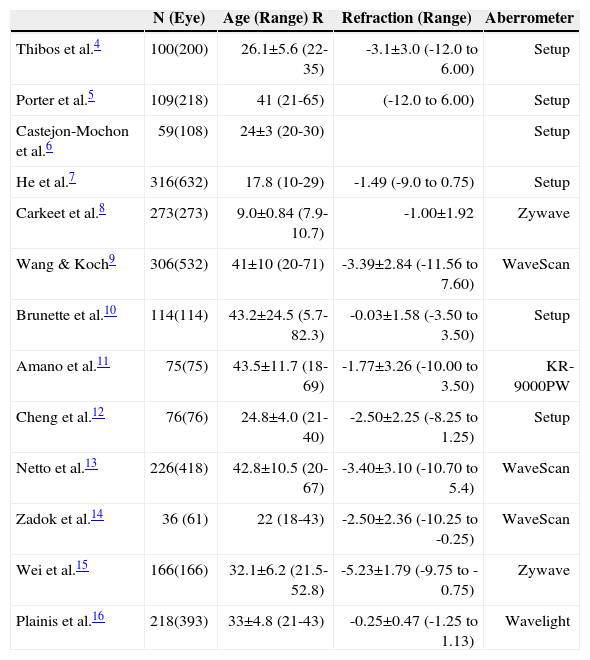
However, besides the three aforementioned laboratory studies,4-6 several other wavefront measurements with a large sample size have also been recently documented in the literature.7-16Table 1 summarizes the basic information on sample size, age, refraction and techniques used in each of the studies. In those later studies, five of them7-9,15-16 reported mean Zernike coefficients, and four experiments were conducted using commercial aberrometers. Carkeet and colleagues8 statistically tested the mean of the higher-order Zernike aberrations (3rd to 5th order), and found 10 out of 15 Zernike terms to be significantly different from zero. Taking the mean Zernike coefficients and standard deviations reported by Wang and Koch9 and by Wei et al.15 as starting point, we have made a statistical test using their data with multi-comparison correction and found that about 2/3 of the Zernike terms were significantly different from zero. Plainis and Pallikaris16 only reported mean higher-order Zernike aberrations taking the right and left eyes separately. A reanalysis of their data with multi-comparison correction revealed that three higher-order Zernike terms, including spherical aberration, were significantly different from zero when both eyes were averaged together. Obviously, the hypothesis stating that human eyes show a central tendency to be free of higher-order aberrations was not supported in the four later population studies.8-9,15-16
Information regarding number of subjects N, mean ±SD of age (year), mean ±SD of refractive error (D) and aberrometers used in previous population studies. “Setup” under “aberrometer” means experimental setup
| N (Eye) | Age (Range) R | Refraction (Range) | Aberrometer | |
| Thibos et al.4 | 100(200) | 26.1±5.6 (22-35) | -3.1±3.0 (-12.0 to 6.00) | Setup |
| Porter et al.5 | 109(218) | 41 (21-65) | (-12.0 to 6.00) | Setup |
| Castejon-Mochon et al.6 | 59(108) | 24±3 (20-30) | Setup | |
| He et al.7 | 316(632) | 17.8 (10-29) | -1.49 (-9.0 to 0.75) | Setup |
| Carkeet et al.8 | 273(273) | 9.0±0.84 (7.9-10.7) | -1.00±1.92 | Zywave |
| Wang & Koch9 | 306(532) | 41±10 (20-71) | -3.39±2.84 (-11.56 to 7.60) | WaveScan |
| Brunette et al.10 | 114(114) | 43.2±24.5 (5.7-82.3) | -0.03±1.58 (-3.50 to 3.50) | Setup |
| Amano et al.11 | 75(75) | 43.5±11.7 (18-69) | -1.77±3.26 (-10.00 to 3.50) | KR-9000PW |
| Cheng et al.12 | 76(76) | 24.8±4.0 (21-40) | -2.50±2.25 (-8.25 to 1.25) | Setup |
| Netto et al.13 | 226(418) | 42.8±10.5 (20-67) | -3.40±3.10 (-10.70 to 5.4) | WaveScan |
| Zadok et al.14 | 36 (61) | 22 (18-43) | -2.50±2.36 (-10.25 to -0.25) | WaveScan |
| Wei et al.15 | 166(166) | 32.1±6.2 (21.5-52.8) | -5.23±1.79 (-9.75 to -0.75) | Zywave |
| Plainis et al.16 | 218(393) | 33±4.8 (21-43) | -0.25±0.47 (-1.25 to 1.13) | Wavelight |
Yet, there were differences between these four later studies8-9,15-16 and the three early laboratory studies,4-6 such as the systems used to measure aberrations, subject age and refraction, and even the usage of cycloplegia. While the experimental systems for the three early studies were constructed in the laboratory, the aberrometers used in the four later studies were commercial models. It is quite possible that different systems might have different accuracy and precision, thus resulting in different data.
In order to test the hypothesis of a population having eyes free of higher-order aberrations, we have measured the wavefront aberrations for a group of young adults using a commercial aberrometer (WASCA Wave-front Analyzer), which has been experimentally tested for its accuracy and precision in a previous study.17 For a better understanding of the nature of higher-order aberrations in a normal population, this study was focused on emmetropes, because it is more reasonable to test the hypothesis in normal emmetropic eyes rather than in eyes with refractive errors. The subjects in the study of Plainis & Pallikaris16 were emmetropes also, but only three higher-order Zernike aberrations were found to be statistically different from zero. In addition, we have also tested a group of young myopes for comparison. Moreover, wavefront aberrations in the anterior corneal surface were examined using a precisely calibrated corneal topography system,18,19 because the anterior cornea plays an important role in determining wavefront aberrations in the whole eye.18,20-23
MethodSubjectsEmmetropic subjects were recruited among students of the Wenzhou Medical College (WMC) and among students from the Wenzhou police school. Myopic subjects were recruited from the WMC and the candidates for refractive surgery in the Refractive Surgery Center of Eye hospital, WMC. Best corrected visual acuity (BCVA) for all subjects was 20/25 or better. Subjects with any ocular pathology or having astigmatism greater than 2.5D were excluded. The final subject number in this study was 75 in the emmetropic group and 196 in the myopic group.
Refraction was measured with the use of cycloplegia. The emmetropes were aged 18 to 33 yrs (mean = 21.73.4 yrs) and had spherical errors ranging from -0.50 to +1.25 D (mean = 0.13±0.37D), including the subjects with -0.5D in only one eye, and cylinder from -2.00 to 0.00D (mean = -0.36±0.29D). Only one subject had spherical error equal to 1.25D, and the rest had values equal or less than 0.75D. The myopes were aged 18 to 38 yrs (mean = 25.2±5.0 yrs), and had spherical errors ranging from -10.0 to -0.5D (mean = -4.70±2.14 D), including the subjects that had -0.5D in both eyes, and a cylinder from -2.50 to 0.00D (mean = -0.64±0.56D). The research followed the tenets of the Declaration of Helsinki, and was approved by the Committee of Ethics of Wenzhou Medical College.
InstrumentsA Humphrey ATLAS Corneal Topography System (Carl Zeiss Meditec, Germany) was used to measure corneal aberrations. The system directly provided estimates of the pupil margin, pupil center location, vertex location, curvatures of the anterior corneal surface, and keratometric measurements. We have used the corneal curvatures and corneal heights, exported from the ATLAS system, to calculate corneal aberrations. Wavefront aberrations in the whole eye were measured using a WASCA Wavefront Analyzer (Carl Zeiss Meditec, Germany), from which refractive error and a series of Zernike aberration terms, up to 7th order, were directly obtained. According to Salmon et al.’s study,17 the repeatability of the WASCA system for 3rd, 4th, 5th, 6th and 7th order aberrations were 0.035, 0.025, 0.020, 0.015 and 0.010 μm respectively.
Experimental ProcedureThe experiment was performed with room lights off. No mydriatics were used. For each subject, four corneal topographies over a 10.0mm zone were taken first, followed by three measurements of the wavefront aberrations of the whole eye. Most subjects had a pupil size greater than 6.0mm during the measurements of whole-eye aberrations. For those subjects whose pupil size was less than 6.0mm, the data was excluded from further analysis. The right and left eyes were tested in random order, and for each subject it took about 10 minutes to complete the experiments.
Data AnalysisFrom the corneal heights, exported from the ATLAS system, wavefront aberrations for the anterior cornea were calculated using a customized MatLab ray-tracing program18-19 to derive Zernike aberration terms up to the 7th order (35 terms). The corneal height data were originally referenced to corneal vertex in the ATLAS system. In order to describe the corneal aberrations with respect to the line of sight of the eye, as it is done for the whole-eye aberrations, a transformation of the coordinate center from the corneal vertex to the pupil center was performed with the customized program, using the pupil center measurements provided by the ATLAS system. After the transformation, corneal height data over a 6.0mm diameter area, relative to the pupil center, were used to calculate corneal Zernike aberrations with ray-tracing and Gram-Schmidt orthogonalization procedures.18 For each eye, the mean of three measurements of either the anterior cornea or the whole eye over a 6.0mm pupil area was calculated and taken as the final estimate of the aberrations. The single-index conversion was used to name the Zernike aberrations.24 Statistical analyses were performed using SPSS 13.0.
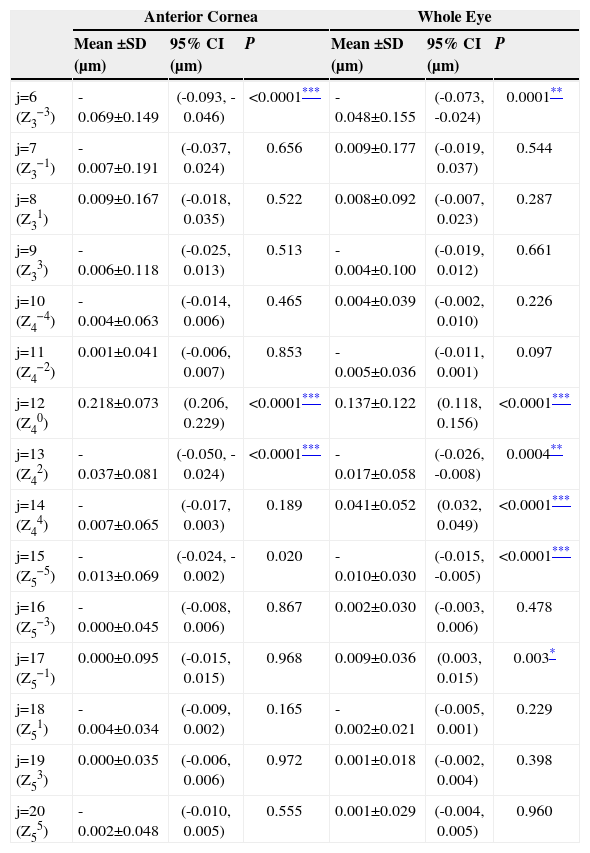
ResultsMean Higher-Order Zernike Aberrations for EmmetropesWhen both the right and the left eyes were accounted together, the resulting mean signed Zernike aberrations in the anterior cornea and the whole eye for 75 emmetropic subjects are as listed in table 2, where only 3rd to 5th orders were included. All other higher order aberrations (6th to 7th) were not given in table 2 because the mean absolute values or magnitudes were very small (< 0.01μm). The results of the t-test at a 95% confidence interval and P-value (uncorrected for multi-comparison) for the mean values being different from zero are also listed in table 2. Significance corrected for multi-comparison was indicated with asterisks for the corresponding levels. As depicted in table 2, three Zernike terms (j=6, 12 and 13) were significantly different from zero in both the anterior cornea and the whole eye simultaneously. Three additional modes (j=14, 15 and 17) were different from zero only in the whole eye. While the spherical aberration (j=12) both in the anterior cornea and in the whole eye was positive, the aberration coefficients corresponding to j=6 and 13 were always negative. The absolute values in the anterior cornea were always greater than those in the whole eye for these three Zernike aberrations (j=6, 12 and 13). For the three non-zero Zernike aberrations in the whole eye only, the mean amplitude of the 4th order aberration (j=14) was relatively large (>0.04μm) while the levels of the other two 5th order terms (j=15 and 17) were around or less than 0.01μm.
Mean higher-order Zernike aberrations of the anterior cornea and of the whole eye over a 6.0 mm pupil area for 76 young emmetropes, with signed coefficients from both right and left eyes averaged together
| Anterior Cornea | Whole Eye | |||||
| Mean ±SD (μm) | 95% CI (μm) | P | Mean ±SD (μm) | 95% CI (μm) | P | |
| j=6 (Z3−3) | -0.069±0.149 | (-0.093, -0.046) | <0.0001*** | -0.048±0.155 | (-0.073, -0.024) | 0.0001** |
| j=7 (Z3−1) | -0.007±0.191 | (-0.037, 0.024) | 0.656 | 0.009±0.177 | (-0.019, 0.037) | 0.544 |
| j=8 (Z31) | 0.009±0.167 | (-0.018, 0.035) | 0.522 | 0.008±0.092 | (-0.007, 0.023) | 0.287 |
| j=9 (Z33) | -0.006±0.118 | (-0.025, 0.013) | 0.513 | -0.004±0.100 | (-0.019, 0.012) | 0.661 |
| j=10 (Z4−4) | -0.004±0.063 | (-0.014, 0.006) | 0.465 | 0.004±0.039 | (-0.002, 0.010) | 0.226 |
| j=11 (Z4−2) | 0.001±0.041 | (-0.006, 0.007) | 0.853 | -0.005±0.036 | (-0.011, 0.001) | 0.097 |
| j=12 (Z40) | 0.218±0.073 | (0.206, 0.229) | <0.0001*** | 0.137±0.122 | (0.118, 0.156) | <0.0001*** |
| j=13 (Z42) | -0.037±0.081 | (-0.050, -0.024) | <0.0001*** | -0.017±0.058 | (-0.026, -0.008) | 0.0004** |
| j=14 (Z44) | -0.007±0.065 | (-0.017, 0.003) | 0.189 | 0.041±0.052 | (0.032, 0.049) | <0.0001*** |
| j=15 (Z5−5) | -0.013±0.069 | (-0.024, -0.002) | 0.020 | -0.010±0.030 | (-0.015, -0.005) | <0.0001*** |
| j=16 (Z5−3) | -0.000±0.045 | (-0.008, 0.006) | 0.867 | 0.002±0.030 | (-0.003, 0.006) | 0.478 |
| j=17 (Z5−1) | 0.000±0.095 | (-0.015, 0.015) | 0.968 | 0.009±0.036 | (0.003, 0.015) | 0.003* |
| j=18 (Z51) | -0.004±0.034 | (-0.009, 0.002) | 0.165 | -0.002±0.021 | (-0.005, 0.001) | 0.229 |
| j=19 (Z53) | 0.000±0.035 | (-0.006, 0.006) | 0.972 | 0.001±0.018 | (-0.002, 0.004) | 0.398 |
| j=20 (Z55) | -0.002±0.048 | (-0.010, 0.005) | 0.555 | 0.001±0.029 | (-0.004, 0.005) | 0.960 |
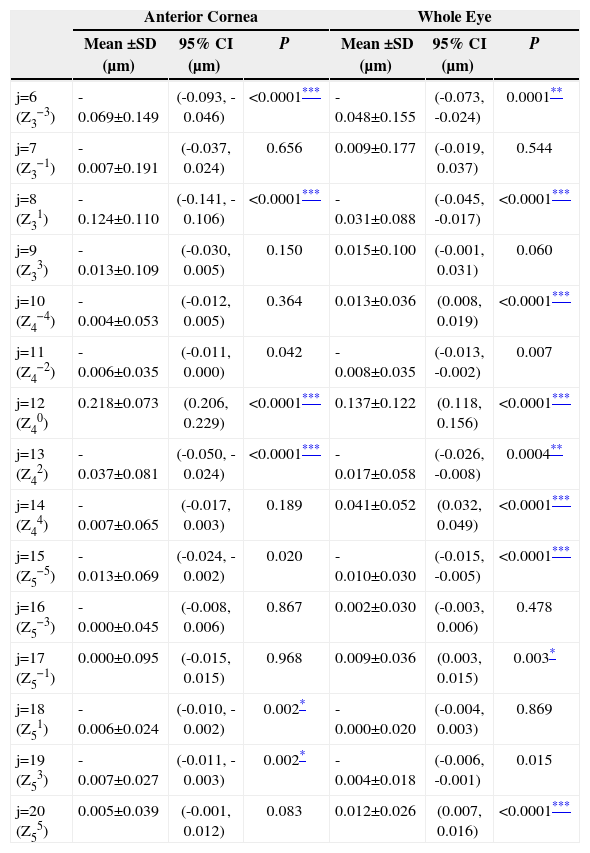
Bilateral symmetry of wavefront aberrations between the right and left eyes both in the anterior cornea and in the whole eye has been well documented in literature.5-6,9,13,23,25-30 With bilateral symmetrical structure, the sign of Zernike coefficients in the right eye is opposite to that in the left eye for those Zernike terms that are asymmetrical with respect to the y-axis, those corresponding to j=8, 9, 10, 11, 18, 19 and 20. To account for the effect of bilateral symmetry on statistical analysis, the sign in the left eye is usually flipped before an average of the two eyes was made. Table 3 shows the mean Zernike aberrations for the emmetropes with the signs in the left eye flipped. Because the sign flipping was restricted to the seven y-axis asymmetrical terms, the results in Table 3 therefore differ from those in Table 2 only in these seven terms. As shown in Table 3, three more terms in either the cornea (j=8, 18 and 19) or the whole eye (j=8, 10 and 20) become significantly different from zero.
Mean-higher order Zernike aberrations of the anterior cornea and of the whole eye over a 6.0mm pupil area for 76 young emmetropes, with signed coefficients averaged for both right and left eyes but the signs flipped for the y-axis asymmetrical Zernike coefficients in the left eye
| Anterior Cornea | Whole Eye | |||||
| Mean ±SD (μm) | 95% CI (μm) | P | Mean ±SD (μm) | 95% CI (μm) | P | |
| j=6 (Z3−3) | -0.069±0.149 | (-0.093, -0.046) | <0.0001*** | -0.048±0.155 | (-0.073, -0.024) | 0.0001** |
| j=7 (Z3−1) | -0.007±0.191 | (-0.037, 0.024) | 0.656 | 0.009±0.177 | (-0.019, 0.037) | 0.544 |
| j=8 (Z31) | -0.124±0.110 | (-0.141, -0.106) | <0.0001*** | -0.031±0.088 | (-0.045, -0.017) | <0.0001*** |
| j=9 (Z33) | -0.013±0.109 | (-0.030, 0.005) | 0.150 | 0.015±0.100 | (-0.001, 0.031) | 0.060 |
| j=10 (Z4−4) | -0.004±0.053 | (-0.012, 0.005) | 0.364 | 0.013±0.036 | (0.008, 0.019) | <0.0001*** |
| j=11 (Z4−2) | -0.006±0.035 | (-0.011, 0.000) | 0.042 | -0.008±0.035 | (-0.013, -0.002) | 0.007 |
| j=12 (Z40) | 0.218±0.073 | (0.206, 0.229) | <0.0001*** | 0.137±0.122 | (0.118, 0.156) | <0.0001*** |
| j=13 (Z42) | -0.037±0.081 | (-0.050, -0.024) | <0.0001*** | -0.017±0.058 | (-0.026, -0.008) | 0.0004** |
| j=14 (Z44) | -0.007±0.065 | (-0.017, 0.003) | 0.189 | 0.041±0.052 | (0.032, 0.049) | <0.0001*** |
| j=15 (Z5−5) | -0.013±0.069 | (-0.024, -0.002) | 0.020 | -0.010±0.030 | (-0.015, -0.005) | <0.0001*** |
| j=16 (Z5−3) | -0.000±0.045 | (-0.008, 0.006) | 0.867 | 0.002±0.030 | (-0.003, 0.006) | 0.478 |
| j=17 (Z5−1) | 0.000±0.095 | (-0.015, 0.015) | 0.968 | 0.009±0.036 | (0.003, 0.015) | 0.003* |
| j=18 (Z51) | -0.006±0.024 | (-0.010, -0.002) | 0.002* | -0.000±0.020 | (-0.004, 0.003) | 0.869 |
| j=19 (Z53) | -0.007±0.027 | (-0.011, -0.003) | 0.002* | -0.004±0.018 | (-0.006, -0.001) | 0.015 |
| j=20 (Z55) | 0.005±0.039 | (-0.001, 0.012) | 0.083 | 0.012±0.026 | (0.007, 0.016) | <0.0001*** |
Root-mean-square (RMS) of the higher-order aberrations (3rd to 5th orders) for both the right and the left eyes were calculated for the 75 emmetropes, and the mean RMS for all 150 eyes was equal to 0.411μm in the anterior cornea and to 0.336μm in the whole eye. When spherical aberration was excluded from the RMS calculation, the mean RMS values decreased to 0.337μm and 0.284μm respectively. The RMS of mean higher order aberrations was also calculated according to the mean Zernike values in Table 2 and 3. Without flipping the signs (Table 2), the RMS of higher-order aberration terms was equal to 0.233μm (in the cornea) and 0.155μm (in the whole eye) when spherical aberration was included, and 0.079μm (in the cornea) and 0.070μm (in the whole eye) when spherical aberration was excluded. After the signs were flipped, the higher-order RMS values became 0.264μm (in the cornea) and 0.159μm (in the whole eye) with spherical aberration included, and 0.147μm (in the cornea) and 0.080μm (in the whole eye) when spherical aberration was excluded.
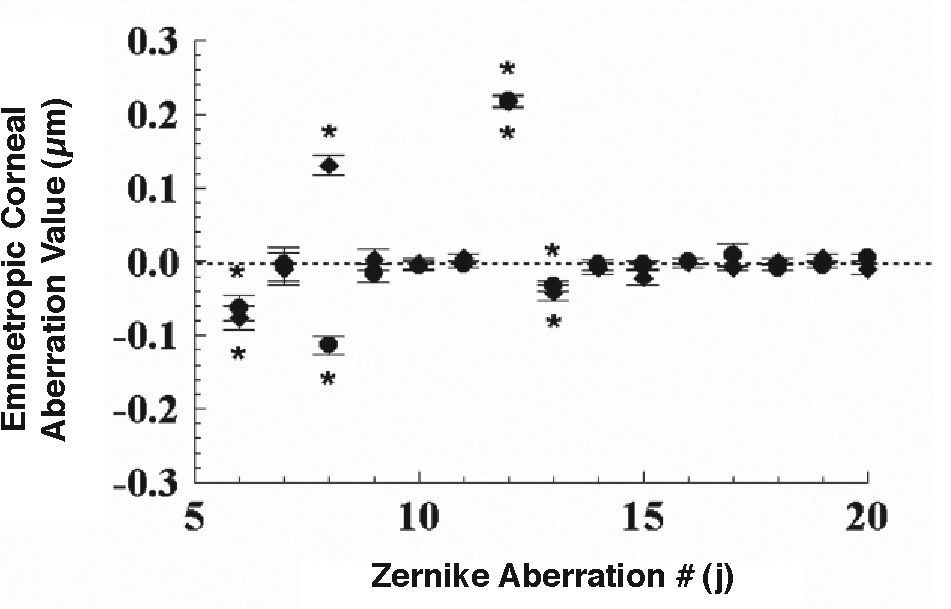
Figure 1 shows the mean corneal Zernike aberrations in the right (solid circles) and the left eye (solid diamond) for the 75 emmetropes, with the error bars standing for ±one standard error of the mean, when the data from the two eyes was analyzed separately. There were 4 Zernike terms significantly different from zero: those corresponding to j = 6 (t=3.56, P=0.0006 for OD; t=4.55, P=0.0002 for OS), 8 (t=9.03, P<0.0001 for OD; t=9.68, P<0.0001 for OS), 12 (t=27.46, P<0.0001 for OD; t=24.63, P<0.0001 for OS) and 13 (t=4.39, P<0.0001 for OD; t=3.86, P=0.0002 for OS) both for the right and left eyes. The horizontal coma (j=8) was significantly different between the right and left eyes also (t=13.24, P<0.0001). It can be seen in figure 1 that the mean magnitude of the horizontal coma (-0.11±0.11μm for OD and 0.13±0.12μm for OS) is large compared to other higher-order aberrations, except of the spherical aberration (0.22±0.07μm for OD and 0.22±0.08μm for OS).
 and left eyes (solid diamonds) of 76 emmetropes.")
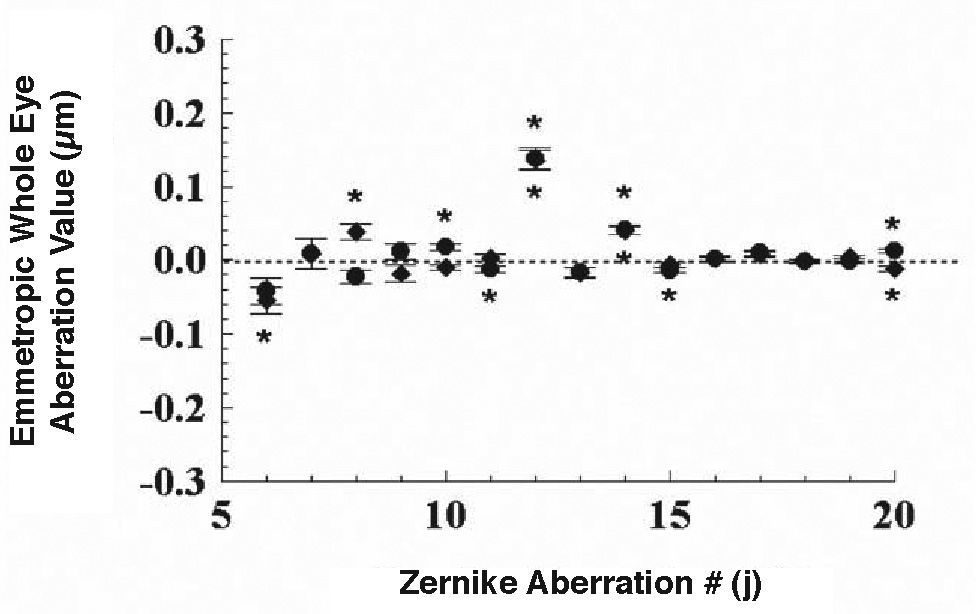
Figure 2 shows the mean higher-order Zernike aberrations in the whole eye for the 75 emmetropes with the two eyes analyzed separately. Six terms in the right eye were significantly different from zero, those being j= 10 (t=4.28, P<0.0001), 11 (t=3.10, P=0.003), 12 (t=9.83, P<0.0001), 14 (t=6.61, P<0.0001), 15 (t=4.05, p=0.0001) and 20 (t=4.20, P<0.0001), but the mean amplitude of four of them (j=10, 11, 15 and 20) was around 0.01μm. In the left eye, five terms were found to be significantly different from zero: j=6 (t=3.10, P=0.003), 8 (t=3.70, P=0.0004), 12 (t=9.74, P<0.0001), 14 (t=6.92, P<0.0001), and 20 (t=3.69, P=0.0004). Only j=20 had a mean amplitude of around 0.01μm, the rests were much higher in amplitude (>0.035μm). The terms showing significantly different values between the two eyes were j=8 (t=4.31, P<0.0001) and 10 (t=4.65, P<0.0001).
Mean Higher Order Zernike Aberrations for Myopes and left eyes (solid diamonds) of 76 emmetropes.")
Mean higher order aberrations in the anterior cornea and the whole eye for 196 myopes were calculated by averaging the aberrations across the right and left eyes. Instead of 3 terms, as shown for the emmetropes in Table 2, 8 corneal Zernike modes were found to be significantly different from zero for the myopes, and those were j = 6, 7, 11, 12, 14, 16, 17, and 20. For the whole eye, 5 terms (j = 10, 12, 14, 15, and 16) were significantly different from zero. Three nonzero aberration terms, j = 12, 14 and 16, in both the anterior cornea and the whole eye were observed. As in the emmetropic group, mean spherical aberration in the myopic group was positive both for the anterior cornea and for the whole eye, but with greater amplitude in the cornea than in the whole eye. Unlike the emmetropic group, the mean aberration of j=6 in the whole eye for the myopic group was not significantly different from zero. All the non-zero aberrations in the 5th order were very small in amplitude (<=0.01μm).
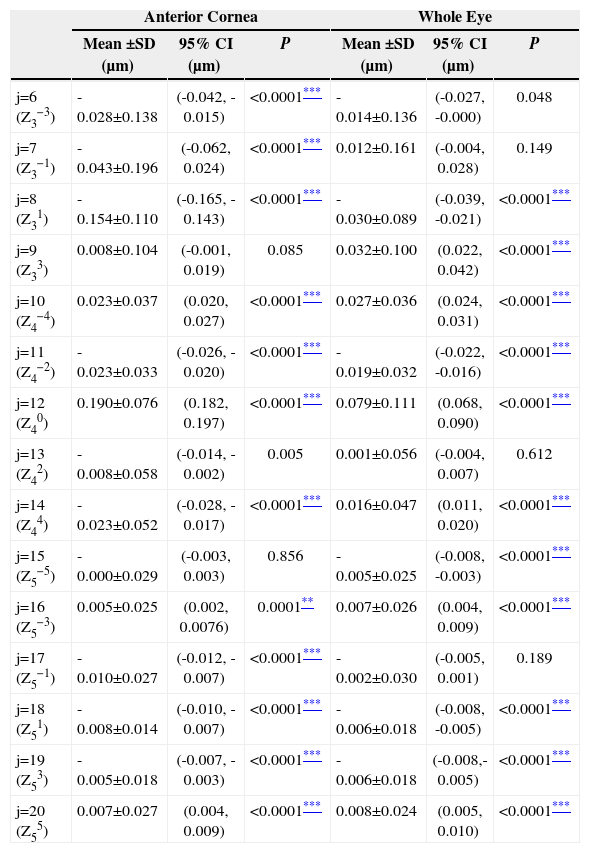
Table 4 shows the mean Zernike aberrations for the myopes, but where the signs corresponding to the left eye have been flipped. Once the signs were flipped, only three (j=9, 13 and 15) out of the 15 terms in the cornea and four (j=6, 7, 13 and 17) out of the 15 terms in the whole eye were not significantly different from zero.
Mean higher-order Zernike aberrations of the anterior cornea and of the whole eye over a 6 mm pupil area for 196 young myopes, with signed coefficients averaged for both the right and left eyes but the signs flipped for the y-axis asymmetrical Zernike coefficients in the left eye
| Anterior Cornea | Whole Eye | |||||
| Mean ±SD (μm) | 95% CI (μm) | P | Mean ±SD (μm) | 95% CI (μm) | P | |
| j=6 (Z3−3) | -0.028±0.138 | (-0.042, -0.015) | <0.0001*** | -0.014±0.136 | (-0.027, -0.000) | 0.048 |
| j=7 (Z3−1) | -0.043±0.196 | (-0.062, 0.024) | <0.0001*** | 0.012±0.161 | (-0.004, 0.028) | 0.149 |
| j=8 (Z31) | -0.154±0.110 | (-0.165, -0.143) | <0.0001*** | -0.030±0.089 | (-0.039, -0.021) | <0.0001*** |
| j=9 (Z33) | 0.008±0.104 | (-0.001, 0.019) | 0.085 | 0.032±0.100 | (0.022, 0.042) | <0.0001*** |
| j=10 (Z4−4) | 0.023±0.037 | (0.020, 0.027) | <0.0001*** | 0.027±0.036 | (0.024, 0.031) | <0.0001*** |
| j=11 (Z4−2) | -0.023±0.033 | (-0.026, -0.020) | <0.0001*** | -0.019±0.032 | (-0.022, -0.016) | <0.0001*** |
| j=12 (Z40) | 0.190±0.076 | (0.182, 0.197) | <0.0001*** | 0.079±0.111 | (0.068, 0.090) | <0.0001*** |
| j=13 (Z42) | -0.008±0.058 | (-0.014, -0.002) | 0.005 | 0.001±0.056 | (-0.004, 0.007) | 0.612 |
| j=14 (Z44) | -0.023±0.052 | (-0.028, -0.017) | <0.0001*** | 0.016±0.047 | (0.011, 0.020) | <0.0001*** |
| j=15 (Z5−5) | -0.000±0.029 | (-0.003, 0.003) | 0.856 | -0.005±0.025 | (-0.008, -0.003) | <0.0001*** |
| j=16 (Z5−3) | 0.005±0.025 | (0.002, 0.0076) | 0.0001** | 0.007±0.026 | (0.004, 0.009) | <0.0001*** |
| j=17 (Z5−1) | -0.010±0.027 | (-0.012, -0.007) | <0.0001*** | -0.002±0.030 | (-0.005, 0.001) | 0.189 |
| j=18 (Z51) | -0.008±0.014 | (-0.010, -0.007) | <0.0001*** | -0.006±0.018 | (-0.008, -0.005) | <0.0001*** |
| j=19 (Z53) | -0.005±0.018 | (-0.007, -0.003) | <0.0001*** | -0.006±0.018 | (-0.008,-0.005) | <0.0001*** |
| j=20 (Z55) | 0.007±0.027 | (0.004, 0.009) | <0.0001*** | 0.008±0.024 | (0.005, 0.010) | <0.0001*** |
Significance was corrected for multi-comparison with * standing for P<0.05 (0.0033)
Mean RMS value for all 392 myopic eyes was 0.389μm in the anterior cornea and 0.291μm in the whole eye. With spherical aberration excluded, the mean RMS values decreased to 0.326μm and 0.258μm in the anterior cornea and in whole eye, respectively. Without flipping the signs, the RMS value associated to the mean higher-order Zernike aberrations was 0.199μm (in the cornea) and 0.084μm (in the whole eye) when spherical aberration was included, and 0.061μm (in the cornea) and 0.028μm (in the whole eye) when spherical aberration was excluded. Once the signs were flipped, the RMS value associated to the mean higher-order Zernike aberrations went up to 0.254μm (in the cornea) and 0.101μm (in the whole eye) with spherical aberration included, and 0.169μm (in the cornea) and 0.062μm (in the whole eye) with spherical aberration excluded.
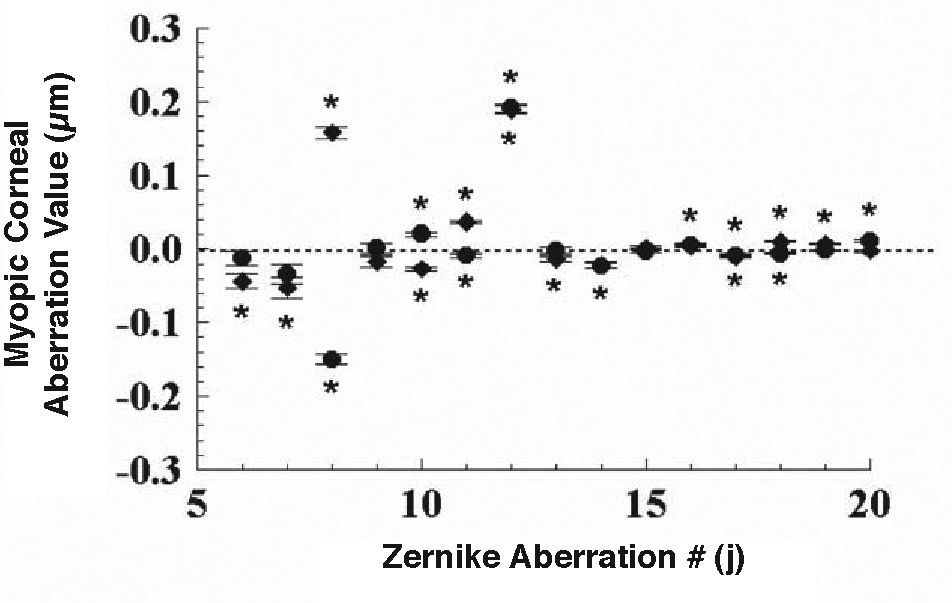
Figure 3 shows the mean higher-order Zernike aberration terms in the anterior cornea for the right (solid circles) and left eyes (solid diamonds) of the 196 myopic subjects. Nine out of the 15 Zernike aberration terms corresponding to the right eye were significantly deviated from zero, among them eight (j = 8, 10, 11, 12, 14, 17, 18, and 20) had a t-test value greater than 4.15 (P<0.0001). Another one j = 16 had a t value equal to 3.23 (P=0.0015). As for the left eye, eleven Zernike terms (j = 6, 7, 8, 10, 11, 12, 13, 14, 17, 18, and 19) were significantly different from zero, and most of them had a t value greater than 4.30 (P<0.0001) except for j = 7 and 13, which had a t value between 3.5 and 3.8 (P<0.001). Meanwhile, six terms (j = 8, 10, 11, 18, 19, and 20) were significantly different when comparing left and right eyes, with t value being greater than 5.0 (P<0.0001).
 and left eyes (solid diamonds) of 196 myopes.")
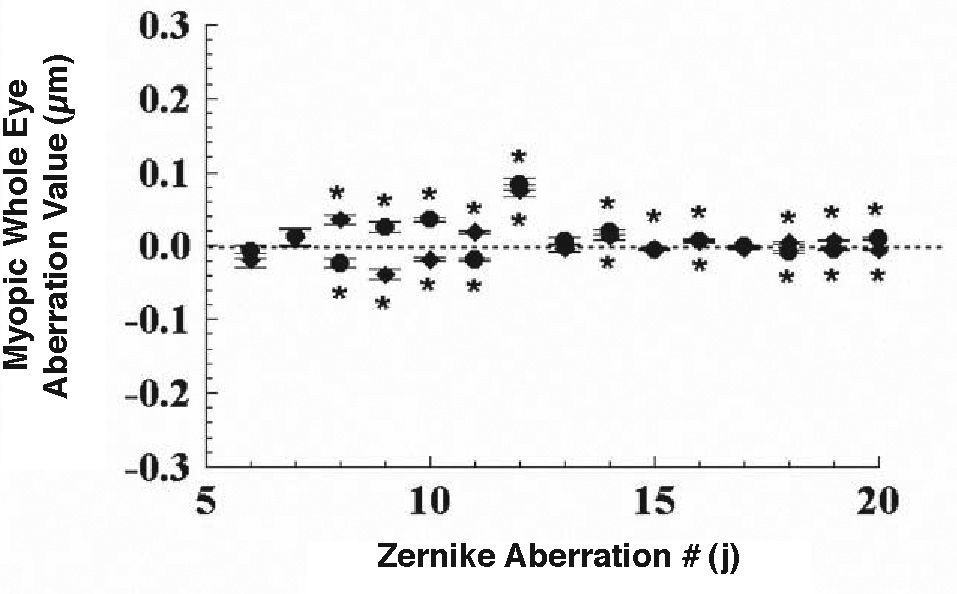
Figure 4 shows the mean higher-order Zernike aberration terms corresponding to the whole eye in both the right and left eyes for the 196 young myopes. Eleven out of the fifteen Zernike aberrations were different from zero in the right eye, and seven of them (j = 10, 11, 12, 14, 16, 18, and 20) had t values greater than 4.07 (P<0.0001). The other 4 terms (j = 8, 9, 15, and 19) had t values that ranged from 3.55 to 3.82 (P<0.001). Ten Zernike aberrations in the left eye were significantly different from zero, and six of them (j = 8, 9, 10, 11, 12, and 19) had t values greater than 5.48 (P<0.0001). The other 4 terms (j = 14, 16, 18, and 20) had t values between 3.13 and 3.65 (P<0.003). For seven higher-order aberration terms the values for the right and left eyes differed significantly: j = 8, 9, 10, 11, 18, 19, and 20 (t > 6.3, P<0.0001 for all of them).
Discussion and left eyes (solid diamonds) of 196 myopes.")
We have found that five out of the fifteen higher-order Zernike aberrations (3rd to 5th orders) in the whole eye of 75 young emmetropes, in addition to the spherical aberration, had mean levels significantly different from zero when signed Zernike aberrations were averaged across the right and left eyes of the same individual (Table 2). Three more terms become statistically different from zero as the signs of y-axis asymmetrical Zernike aberrations in the left eye were flipped (Table 3). The results indicate that, on average, the emmetropic population is not free from higher-order Zernike aberrations. This is consistent with the study on emmetropes by Plainis and Pallikris16 (with three statically non-zero terms including spherical aberration), although in this study more higherorder terms (six terms) were found to be statistically non-zero. Regarding the mean RMS associated to higher-order aberrations for all emmetropes (0.336μm with spherical aberration and 0.284μm without spherical aberration), the RMS of the mean Zernike higher-order aberrations of the emmetropic group was about 46% (0.155/0.336 with spherical aberration) and 25% (0.07/0.284 without spherical aberration) in amount respectively when sign was not flipped, and 47% (0.159/0.336 with spherical aberration) and 28% (0.080/0.284 without spherical aberration) respectively when sign was flipped. The results suggests that the mean higher-order Zernike aberrations in a young emmetropic population are not small and, thus, should not be overlooked. Therefore, the human eye, even in the best case of emmetropia, has not reached yet the condition of being free of higher-order aberrations.
Regarding to the whole eye aberrations for the myopic group, five higher-order Zernike terms, including spherical aberration, were statistically non-zero when signs were not flipped, increasing to eleven terms that were statistically non-zero when the signs were flipped (Table 4). The number of statistically non-zero Zernike aberrations for the myopic group was, in this study, very close to the value obtained for the emmetropic group. The subjects in Wang and Koch's9 study were basically myopes and also from an older age, as compared to the subjects in this study. They found that 2/3 of the higher-order Zernike terms were statistically non-zero when the signs were not flipped, which is more than what was observed in this study (5 terms). This might be due to an age difference. But, Carkeet and colleagues8 also found 2/3 statistically non-zero higher-order terms in their subjects, who were of a younger age. Apparently, further study is needed in order to clarify this point.
In the three aforementioned early studies they used laboratory-constructed wavefront sensors,4-6 refraction of their subjects was a bit biased towards myopia, with refractive errors compatible both with that of the myopes in the current study and also those in the other two later studies.9,15 However, only spherical aberration was found to be significantly differing from zero. The reasons behind this inconsistency are not clear to us. But, as for Thibos et al's study,4 a possible factor might be that their subject's pupil was dilated while we tested the natural pupil. After dilation, the pupil center could be shifted31-35 and become closer to the line of sight. This shift of the pupil center toward the line of sight could make the structure of higher-order aberrations more symmetrical with respect to the line of sight, thus systematically reducing the values associated to the asymmetric higherorder aberrations of the population under study.
Sign flipping of y-axis asymmetric Zernike aberrations in the left eye resulted in more Zernike terms being statistically different from zero in both the emmetropic and the myopic groups (Tables 3and4). Analysis of the mean Zernike aberrations taking the two eyes of each individual separately also showed more Zernike terms being significantly different from zero (Figures 1-4) as compared to the results when both left and right eyes were analyzed together. The results indicate that more systematical higher-order aberrations are revealed when the right and the left eyes are considered separately. Because the increase in non-zero Zernike terms with the sign flipping or with eye separation is related to the bilateral symmetry occurring between the two eyes, the systematical higher-order aberrations in a given population must be partially determined by factors which also control this bilateral symmetry of the wavefront aberrations between the two eyes. Obviously this is an interesting issue for further study.
Several statistically non-zero higher-order Zernike aberrations in the anterior cornea were observed in either the emmetropic or the myopic group no matter the signs were flipped or not (Tables 2-4). A similar result, without sign flipping, was also reported by Wang et al.36 In our study, some of the non-zero terms were simultaneously observed in both the anterior cornea and the whole eye, such as j=6, 12 and 13 for emmetropes, even without sign flipping (Table 2). The results suggest that the anterior cornea plays an important role in determining the systematical aberrations in the whole eye. Meanwhile, internal optics, including the posterior cornea and the lens, also contribute to the systematical whole-eye aberrations because some of the statistically non-zero Zernike aberration terms were observed in the whole eye but not in the anterior cornea, e.g. j=14, 15 and 17 (Table 2). Wavefront aberrations in the anterior cornea were partially compensated by interior optics.18,20-23 This is true for this study since the amplitude of the Zernike aberration terms for the whole eye was for most terms smaller than that obtained for the anterior cornea alone, especially for the relatively lower-order Zernike terms (3rd to 4th). The RMS values in the whole eye were also reduced. However, the basic distribution of systematical higher-order aberrations in the whole eye did not change much relative to that obtained for the anterior cornea.
A commercial aberrometer was used to measured wholeeye aberrations in this study. It might be concerned that the systematical higher-order aberrations observed in both the emmetropic and the myopic groups were due to instrumental error because the commercial model was as accurate as the laboratory-constructed systems.4-6 This is a problem for all aberrometers available in the market, since so far we have no standard to test the accuracy of the aberrometers against, when it comes to measuring higher-order aberrations. However, in this study, we found that many of the higher-order aberrations were not significantly different from zero in both the anterior cornea and the whole eye simultaneously. Bearing in mind that the corneal aberration pattern was obtained using a different instrument, the coincidence of getting a similar pattern of wavefront aberrations from two different instruments largely suggests that the hypothesis of an instrumental error is quite unlikely.
This study indicates that the population is not free of higher-order aberrations. This means that the human eye has not reached yet the perfect optical condition during the process of evolution. An interesting question, therefore, is whether or not this systematical higher-order aberrations are of some biological significance for the visual performance of the human eye. While visual acuity was found to be improved as the higher-order aberrations were completely corrected in several recent studies with adaptive optics,37-43 aberration as a cue for accommodation was also demonstrated in some subjects.44 Clearly, further studies on this issue are expected. In clinical practices, it might be needed to think more about what the goal should be: to correct wavefront aberrations completely or not, before a fully understanding of the significance of higher-order aberrations in the eye was established.
This study was supported by Chinese National Key, Technologies R&D Program Grant (2004BA720A16) and Zhejiang, Province Key R&D Program Grant (2005C14001).





