

This article aims to demonstrate how a silicone oil bubble can be mistaken for a dislocated intraocular lens. An 80-year-old gentleman was referred by his optometrist with the diagnosis of dislocated IOL in a pseudophakic eye. Eye examination revealed a silicone oil bubble from previous retinal-detachment surgery and that the lens was in-situ. In conclusion, a history of retinal detachment surgery should alert one that an oil bubble can be misinterpreted as a dislocated IOL.
Este artículo se propone demostrar que una burbuja de aceite de silicona se puede confundir con una lente intraocular (LIO) desplazada. Un paciente varón de 80 años vino derivado por el optometrista; el cual le había diagnosticado “LIO desplazada” en un ojo pseudofáquico. La exploración ocular reveló la presencia de una burbuja de aceite de silicona, proveniente de una intervención anterior de desprendimiento de retina; también confirmó que la LIO estaba correctamente colocada. En conclusión, los antecedentes de cirugía de desprendimiento de retina deberían poner sobre aviso al personal sanitario, puesto que una burbuja de aceite de silicona se puede interpretar erróneamente como una LIO desplazada.
Silicone oil is used in ophthalmic surgery to reattach the retina. Unlike air and gas it does not absorb by the surrounding tissue, requiring its removal to prevent complications such as cataract, keratopathy and glaucoma. The optimal period for removal is still subject to debate and should be decided on a case-by-case basis, but it is currently thought to be between 3 and 6 months if the retina is stable.1
Late dislocation of the intraocular lens (IOL) following cataract surgery occurs in 0.2-3% of the cases.2 Risk factors for this complication include pseudoexfoliation, uveitis, trauma, vitrectomy and increased axial length.2
Case ReportAn 80-year-old gentleman was referred in by his optometrist with a ‘slipped lens’ in his right eye, which had previously undergone a phacoemulsification with implantation of an acrylic IOL followed, 6 months later, by retinal detachment repair using 1000-centistoke silicone oil. The silicone oil was subsequently removed and the patient discharged with stable visual acuity (VA) of 6/18 on the right eye and 6/9 on the left one.
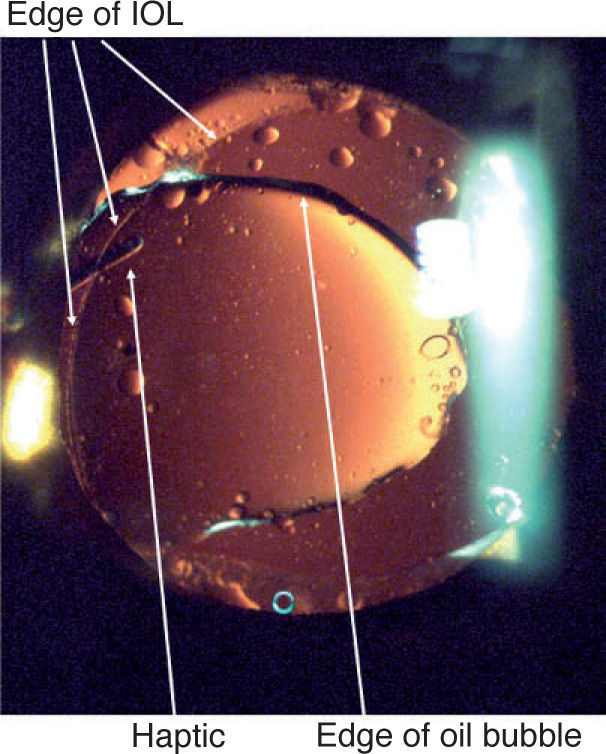
On examination his VA was unchanged, but a silicone oil bubble adherent to the posterior chamber of the IOL was found (Figure 1). Following a full discussion of the risks and benefits of removing the oil bubble the patient opted for a conservative treatment.
Discussion
Silicone oil is a widely used material for retinal detachment surgery and its adherence to IOLs is a well recognised phenomenon.3 Adherence is more likely if the IOL is made of silicone, which is avoided as biomaterial in patients at risk of retinal detachment. Retained silicone oil can emulsify causing floaters, secondary glaucoma and band keratopathy. Therefore, when examining a patient whose appearance suggests a dislocated IOL, it is worth taking a look at their past ocular history. If there is a history of retinal detachment repair, it is worth to include the possibility of a silicone oil bubble in the differential diagnosis.
The authors would like to thank the patient for their permission to publish these images and the photography department at the Oxford Eye Hospital for their imaging expertise.
Financial disclosure: The authors would like to acknowledge that there was no financial or commercial interest involved in the development of this work.





