




A lens coloboma is characterized by the lens tissue's notching at the equator. It is usually inferior-nasal else it is called an atypical coloboma. We report a young male who presented with a superior lens coloboma, an elevation deficit and moderate ptosis, left eye. As superior rectus and levator muscles are derived from the neural crest cell we propose, genetically, there may be an association between the lens coloboma and the superior rectus/levator muscle underaction via an anomalous homeobox gene function.
Un coloboma de cristalino se caracteriza por la presencia de un orificio en el ecuador del tejido del cristalino. Suele ser de tipo inferonasal; en caso contrario se denomina coloboma atípico. Informamos aquí de un varón joven que presentaba en el ojo izquierdo un coloboma de cristalino superior, un déficit de elevación y ptosis moderada. Puesto que el músculo recto y el elevador del párpado se desarrollan a partir de células de la cresta neural, proponemos la hipótesis de que pudiera haber una relación, desde el punto de vista genético, entre el coloboma de cristalino y el mal funcionamiento del músculo recto superior y del elevador, derivado todo de un funcionamiento anómalo de alguno de los genes de homeosecuencia.
A lens coloboma is characterized by its notching at the equator.1 Superior lens coloboma is rare. A lens coloboma is associated with a deficiency or absence of the zonules at that site.1 Colobomas of the lens are divided into typical colobomas (those that occur at the site of the embryonic fissure) and atypical colobomas (not occurring at the site of embryonic fissure).2 We present a case identifying a superior lens coloboma with an elevation deficit and ptosis, proposing a potential genetic association.
Case ReportA 28-year-old man presented to the office with a chief complaint of left eye squint since childhood with accompanying poor vision. Examination uncovered best-corrected acuities of 20/20 for OD and 20/100 for OS. He had significant ptosis in OS measuring +6.0mm with poor levator function.
Cover test uncovered a 45 prism diopter left, constant, noncomitant exotropia, with no accommodative component, deep suppression and severe strabismic amblyopia.
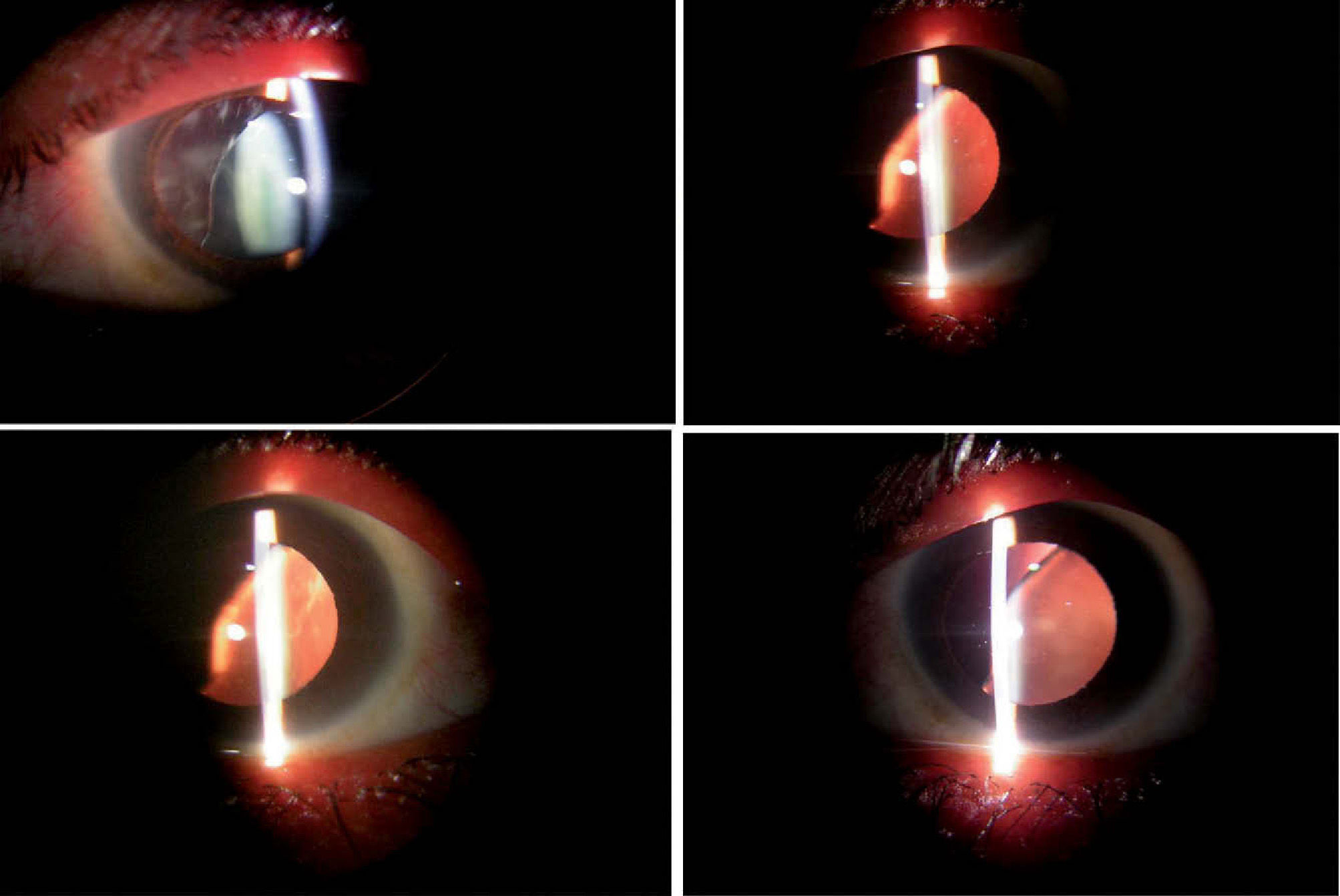
His ocular movements for elevation were restricted both for ductions and versions (-4) (Figure 1). Bell's phenomenon was normal in the patient suggesting intact supranuclear pathways. A forced duction test was positive, suggestive of a tight, restrictive inferior rectus, OS. The forced generation test for the superior rectus was negative. Worth four-dot testing and stereo acuity testing confirmed the presence of deep suppression for OS. Refraction was -0.50 D of sphere, OD and -1.00 -2.50 × 120°, OS, whose correction yielded no improvement in acuity. Biomicroscopy in OS demonstrated a superior- nasal lens coloboma with absent zonules superiorly and nasally (Figure 2) with normal iris architecture. No subluxation was seen. A detailed dilated fundus examination was done and was found to be normal.

We explained our findings regarding both the diagnosed condition and the prognosis for visual potential. We instructed the patient to wear full-time polycarbonate spectacles to attain the best-possible visual results and with the purpose of providing protection for the right eye.
DiscussionA lens coloboma represents an incomplete lens formation due to failure of the fetal fissure to close completely.1 It is often accompanied by other ocular colobomas. It can be seen as a peripheral flattening or indentation of the lens It is usually inferior-nasal.1 It is also usually monocular. Superior-nasal lens coloboma is rare.1-2 A lens coloboma is associated with a deficiency or absence of the zonules at that site.1-2 Colobomas of the lens are divided into typical colobomas (those that occur at the site of the embryonic fissure) and atypical colobomas (not occurring at the site of the embryonic fissure).2 Atypical lens colobomas result from localized deficiencies of zonules that usually occur without an apparent cause. An atypical lens coloboma may follow an adjacent medulloepithelioma or other ciliary body tumor or surgery for congenital glaucoma.3
The embryonic fissure is located inferonasally and closes at the anterior margin (the future equator) first. With the closure of the embryonic fissure the basic structure of the eye is established.
The embryological basis of atypical coloboma is uncertain; various theories propose that it might be due to the rotation of the fetal fissure or that it may develop as a result of an inflammatory process.4 It may also result from persistence of mesodermal tissue of embryonic vascular origin blocking the forward growth of the neuroectoderm, thus causing a defect in the ciliary body and iris.2
Lens coloboma has been documented to cause an astigmatic refractive error.1-2 In these cases, if a significant refractive error is left uncorrected, refractive, meridional or anisometropic amblyopia may develop as a result. The prognosis of visual recovery in cases where visual disability has occurred will depend upon the time of detection (better prognosis inside the sensitive period) and the willingness of the patient to attempt rehabilitation. Cases involving ptosis, a condition where the eyelid covers the pupil, has the potential to cause amblyopia out of disuse. These cases are more difficult to remedy and will require either a ptosis crutch or surgical repositioning of the blocking eyelid. The prognosis of vision was poor at this age and he was advised to undergo squint surgery followed by ptosis surgery.
Lens coloboma is often a misnomer and might better be called coloboma of the zonules or of the ciliary body, as the process actually involves the segmental notching and contraction of the lens due to an absence of the zonules in that location.5
The zonules fail to form in the anterior secondary vitreous or the marginal bundle of Druault during the 3rd-4th month of gestation, due either to the failure of condensation and differentiation of the vitreous substance or to the failure of the lens to induce such changes.6
Embryologically, the choroid, the superior rectus (SR) and the levator palpebralis superioris (LPS) are derived from the neural crest cells.6 The neural crest cell function may be disrupted due to various genetic and epigenetic influences, leading to disturbances in the development of the choroid, SR and LPS, thus leading to the developmental defect.2,7,8 The presentation of a superior lens coloboma with monocular elevation deficit and ptosis does not fit into any recognized syndrome.
We believe that this could be due to a solitary occurrence suggesting the possibility of a developmental field defect due to various genetic or epigenetic factors, leading to the deficient signaling by the Sonic hedge hog (SHH) and PAX6 gene products, resulting in neural crest cell abnormalities that finally cause the superior lens (ciliary) coloboma, an elevator palsy as well as ptosis.9,10 Fields are those parts of the embryo in which the processes of development of complex structures appropriate to those parts are controlled and coordinated in a spatially ordered, temporally synchronized, and epimorphically hierarchical manner. Disturbances of field development may be corrected or may lead to anomalies of abnormal or incomplete differentiation limited to that particular field.





