





To establish whether the cover test and von Graefe methods are interchangeable in a non-presbyopic and presbyopic population.
MethodsWe performed a prospective study on a sample of 127 non-presbyopic subjects between 20 and 45 years old and 56 presbyopic between 40 and 78 years old. Distance and near vision phoria were measured using the von Graefe method (VG) and cover test (CT). We analyzed the significant differences between methods, their correlation and the agreement between them using the Bland and Altman method.
ResultsFor distance vision, heterophoria values for non-presbyopic subjects were −0.61±1.86Δ with CT and −0.88±2.37Δ with VG, and for presbyopic subjects were −0.56±1.64Δ with CT and −0.85±1.94Δ with VG. For near vision, CT yielded −3.02±3.97Δ, while VG achieved −3.49±4.70Δ in non-presbyopic subjects. For presbyopic subjects these values were −6.05±4.38Δ with CT and −6.29±4.19Δ with VG, respectively. Statistically significant differences between the two methods were observed for all groups analyzed (p<0.05), except for near vision in presbyopic subjects (p>0.05). Coefficient of agreement for non-presbyopic was ±2.97Δ for distance vision and ±6.74Δ at near. For presbyopic patients, this coefficient was ±1.59Δ for distance and ±1.86Δ for near vision.
ConclusionCover test and von Graefe methods have a high level of agreement for both distance and near vision when considering presbyopic subjects. For non-presbyopic patients, the level of agreement is very low. Both methods for measuring heterophoria can only be considered interchangeable for presbyopic patients. For clinical purposes, this implies that any method can be used for measuring heterophoria in presbyopic patients.
Establecer si el “cover test” y el método de von Graefe son intercambiables en la población sin y con presbicia.
MétodosRealizamos un estudio prospectivo en una muestra de 127 sujetos sin presbicia de edades comprendidas entre 20 y 45 años, y 56 sujetos con presbicia de entre 40 y 78 años de edad. Se midieron la foria de cerca y lejos utilizando el método de von Graefe (VG) y el cover test (CT). Analizamos las diferencias significativas entre ambos métodos, así como la correlación y concordancia entre ambos utilizando el método de Bland & Altman.
ResultadosPara la visión de lejos, los valores de heteroforia para los sujetos sin presbicia fueron de -0,61±1,86Δ con CT y de -0,88±2,37Δ con VG y, para los sujetos con presbicia, de -0,56±1,64Δ con CT y de -0,85±1,94Δ con VG. Para la visión de cerca, los valores de CT fueron de -3,02±3,97Δ, mientras que los valores de VG fueron de -3,49±4,7Δ en sujetos sin presbicia. Para los sujetos con presbicia, los valores fóricos fueron de -6,05±4,38Δ con CT y de -6,29±4,19Δ con VG. Se observaron diferencias estadísticamente significativas entre los dos métodos para todos los grupos analizados (p<0,05), excepto para la visión de cerca en sujetos con presbicia (p>0,05). El coeficiente de concordancia para los sujetos sin presbicia fue de ±2,97Δ para la visión de lejos, y de ±6,74Δ para la de cerca. Para los pacientes con presbicia, dicho coeficiente fue de ±1,59Δ para la visión de lejos, y de ±1,86Δ para la de cerca.
ConclusiónEl “cover test” y el método de von Graefe tienen un alto nivel de concordancia para la visión de lejos y cerca, en relación a los sujetos con presbicia. Para sujetos sin presbicia, el nivel de concordancia es muy bajo. Ambos métodos de medición pueden intercambiarse para medir la heteroforia únicamente en pacientes con presbicia. A efectos clínicos, esto implica que puede utilizarse cualquiera de los dos métodos para medir la heteroforia en pacientes con presbicia.
Under normal visual conditions, the interaction between the accommodative and vergence systems allows us to see objects focused and fused, allowing the balance of patient's visual function. If an anomaly is present in any of both systems, the operation of the other can be significantly affected, emerging the accommodative and binocular dysfunctions.1,2 To diagnose these binocular disorders, it is essential to know the patient's heterophoria, both distance and near, as an important part of any ocular examination for the management of accommodative and vergence disorders.
There are several ways to measure heterophoria, including the cover test (CT) and the von Graefe method.3–11 Several studies have shown that each test presents different constraints that must be taken into account when administered. Some authors have shown that the minimum detectable ocular deviation in the cover test is two prism diopters (Δ). However, an experienced examiner is able to detect smaller differences.12,13 Indeed, although the heterophoria measurement by the CT depends largely on the skill of the examiner to detect eye movements, it has been found that the alternating CT using prism neutralization provides excellent repeatability, both within and between examiners.3,14–18 It has also been shown to be a reliable measure even when examiners are inexperienced.19 On the other hand, the technique usually used in clinical practice by several authors is the von Graefe method, which is a subjective test that depends on the subject's response. Several studies on the repeatability of this test compared with other techniques have shown that the von Graefe method is less repeatable than other methods such as the modified Thorington test or the CT.3,8,10,11,17,18,20
Some authors have shown that the CT tends to yield lower heterophoria values than the von Graefe method,21 whilst others have reported that the von Graefe method yields higher esophoric values than the cover test.22 Antona et al.17 and Cebrián et al.18 showed that the difference between CT and von Graefe method increases as mean horizontal phoria increases, both for distance and near vision for non-presbyopic subjects.
Few studies have analyzed the level of agreement between both methods to consider them interchangeable. Antona et al.17 obtained an excessively high coefficient of agreement between CT and von Graefe for both distance and near vision for non-presbyopic subjects. Recently, Cebrián et al.18 have obtained similar results, showing the poor level of agreement between both methods, although they only studied distance vision for non-presybyopic subjects. However, it has not been proven at date if this poor agreement should also be established in a presbyopic population. In fact, most of the available information about heterophoria measurement relates to non-presbyopic patients (for whom the prevalence of binocular vision disorders has been shown quite common23) and there is much less data about the presbyopic population. However, it has been currently shown that binocular vision problems are common in the older adults,24 disorders that may result in reduced stereopsis, which has functional consequences.25 This indicates the importance of the phoria measurement in presbyopic population.
Accordingly, the aim of the present study was to analyze and compare the results of heterophoria measurement obtained from the cover test and the von Graefe method for both distance and near vision in a presbyopic and non-presbyopic population, in order to establish its level of agreement.
Material and methodsWe conducted a study on a clinical sample of 183 consecutive subjects examined at the Optometric Clinic of University of Alicante aged between 20 and 78 years old, with a mean age of 34.24±13.47 years. The study followed the tenets of the Declaration of Helsinki, and informed consent was obtained from all subjects after explanation of the nature of the study. The inclusion criteria consisted of subjects whose visual acuity was 20/20 with the best correction and who did not present ocular motility disorders, strabismus, amblyopia, nystagmus, and no history of eye disease or refractive surgery.
All subjects were given a visual examination, which consisted of several tests, including a refractive exam and an ocular exam by means of biomicroscopy and fundus examination. The patient's self-reported history was collected, noting the possible existence of visual symptoms. Objective refraction was performed by static retinoscopy.26 Subjective examination was conducted by means of a monocular fogging with cross-cylinder, followed by binocular balancing to a standard endpoint of maximum plus for best visual acuity (MPBVA). For near vision examination (40cm), the tentative addition for those patients who required it was calculated taking their age into account,27 and using the positive and negative relative accommodation balance.5
The heterophoria of each subject was determined by two methods, the cover test and the von Graefe technique, both performed using the result of MPBVA for distance and near vision. All measurements were undertaken in primary viewing position. For presbyopic patients, determination of near vision heterophoria was executed using the addition calculated previously. According to the ambient illumination, both methods were determined in the same way so that room lighting was left on and for near measurements, the refraction column lights were added. In addition, due to the possible influence of the prisms on vergence adaptation,28 both techniques were done randomized. In order to avoid any bias in performing the procedures, both methods were executed by two different examiners with several years of experience in phoria measurement procedures, and none of the examiners knew the result of the other method. This allowed avoiding any possible influence on the other examiner so that the results of one examiner were not influenced by the results of the other.
Cover testOnce evaluated the cover–uncover test to rule out the existence of strabismus at distance or near vision, the alternate cover test (ACT) protocol was then performed to evaluate the heterophoria status, alternately occluding eyes and observing eye movement when uncovered,3,7,19,28–30 while using a trial frame. We employed a minimum occlusion time of 5s to minimize the effect of vergence adaptation.19,28,30,31 For objective procedure of prism neutralized ACT, each subject was instructed to fixate on a single letter of 20/30 visual acuity for distance,1 and near vision.1,3,7 Using a prism bar (steps of 1, 2, 3, 4, 5, 6, 8, 10, 12, 14, 16, 18, 20, 25, 30, 35, 40 Δ) held no farther than 1cm the phoria value was midway between the low and high neutral findings using an ACT.3,7
Von Graefe methodA dissociating prism of 6 Δ base up was placed in front of the right eye and a measuring prism (12 Δ base in) before the left eye, using the phoropter. For both distance and near vision, subjects were instructed to fixate at the line of 20/30 visual acuity letters and were told to keep the letters clear all the time.1,10 The examiner then asked the subjects to look at the lower target and requested them to inform the examiner when the upper target appeared just above the lower target. For that, the magnitude of the horizontal prism (12 Δ) was changed in one-diopter steps until subjects saw both aligned images. Three measurements were performed and the mean value obtained.
Data analysis and statisticsSince the aim of our study was to analyze the results for presbyopic and non-presbyopic subjects, we decided to divide the sample into two groups. Presbyopic subjects were defined as those who required the prescription of an addition, so that the sample was divided into 127 non-presbyopic subjects, aged between 20 and 45 years old (26.64±6.27 years) and 56 presbyopic subjects aged between 40 and 78 years old (51.48±8.60 years).
By convention, exo-deviations were expressed with negative sign and eso-deviations with positive sign. None of the variables studied presented a normal distribution (Kolmogorov–Smirnov test, p<0.05), so that we used nonparametric tests for statistical analysis (Wilcoxon signed-rank test to determine whether there were statistically significant differences between the two methods for each of the sample populations, U-Mann–Whitney test for the comparison of heterophoria between presbyopic and non-presbyopic patients, and Spearman's rho coefficient to perform a correlation analysis). Finally, Bland–Altman method32 was used to describe the agreement between the two tests. We used the mean difference (mean differences followed a normal distribution, Kolmogorov–Smirnov test, p>0.05), the standard deviation of the differences (SD), the coefficient of agreement (CA=1.96×SD) and the limits of agreement at the 95% level (mean difference±CA). Data were performed using the SPSS 20.0 statistical package.
ResultsTable 1 shows the descriptive statistics for the 127 non-presbyopic and 56 presbyopic subjects, allowing a comparison of the cover test and the von Graefe method for distance and near vision. The table gives the mean and standard deviation and the median for both tests used, as well as the p-value for each comparison. As can be seen, the mean value obtained for distance vision in non-presbyopic and presbyopic subjects was less than the value of 1 Δ of exophoria. This value increased for near vision with both methods. Furthermore, the exophoria obtained for near vision in presbyopic subjects was greater than that observed in non-presbyopic subjects (p<0.05). In addition, statistically significant differences (p<0.05) were found between the CT and von Graefe method for both distance and near vision in non-presbyopic subjects, and only for distance vision in the group of presbyopic patients. Table 1 also shows that in all cases von Graefe mean values were greater than CT ones and a more exophoric heterophoria mean value was obtained when using the von Graefe method.
Comparison of the cover test and the von Graefe method for distance and near vision in non-presbyopic and presbyopic subjects.
| Mean (Δ) | SD (Δ) | Median (Δ) | IQR | p | |
|---|---|---|---|---|---|
| Distance vision | |||||
| Non-presbyopic subjects (N=127) | |||||
| Cover test | −0.61 | 1.86 | −0.50 | 1.00 | 0.020* |
| von Graefe | −0.88 | 2.37 | −1.00 | 2.00 | |
| Presbyopic subjects (N=56) | |||||
| Cover test | −0.56 | 1.64 | −0.50 | 1.00 | 0.003* |
| von Graefe | −0.85 | 1.94 | −1.00 | 1.91 | |
| Near vision | |||||
| Non-presbyopic subjects (N=127) | |||||
| Cover test | −3.02 | 3.97 | −3.00 | 4.50 | 0.028* |
| von Graefe | −3.50 | 4.70 | −3.66 | 6.00 | |
| Presbyopic subjects (N=56) | |||||
| Cover test | −6.05 | 4.38 | −5.50 | 7.00 | 0.058 |
| von Graefe | −6.28 | 4.19 | −5.83 | 5.58 | |
SD, standard deviation; IQR, interquartile range.
A study of the correlation between the two tests for non-presbyopic subjects showed a strong correlation between the cover test and the von Graefe method, with a rho value of 0.71 for distance vision and 0.66 for near vision, both at p<0.001. For presbyopic patients, the correlation analysis indicated the existence of a very strong correlation, with a rho value of 0.88 for distance vision and 0.97 for near vision (p<0.001).
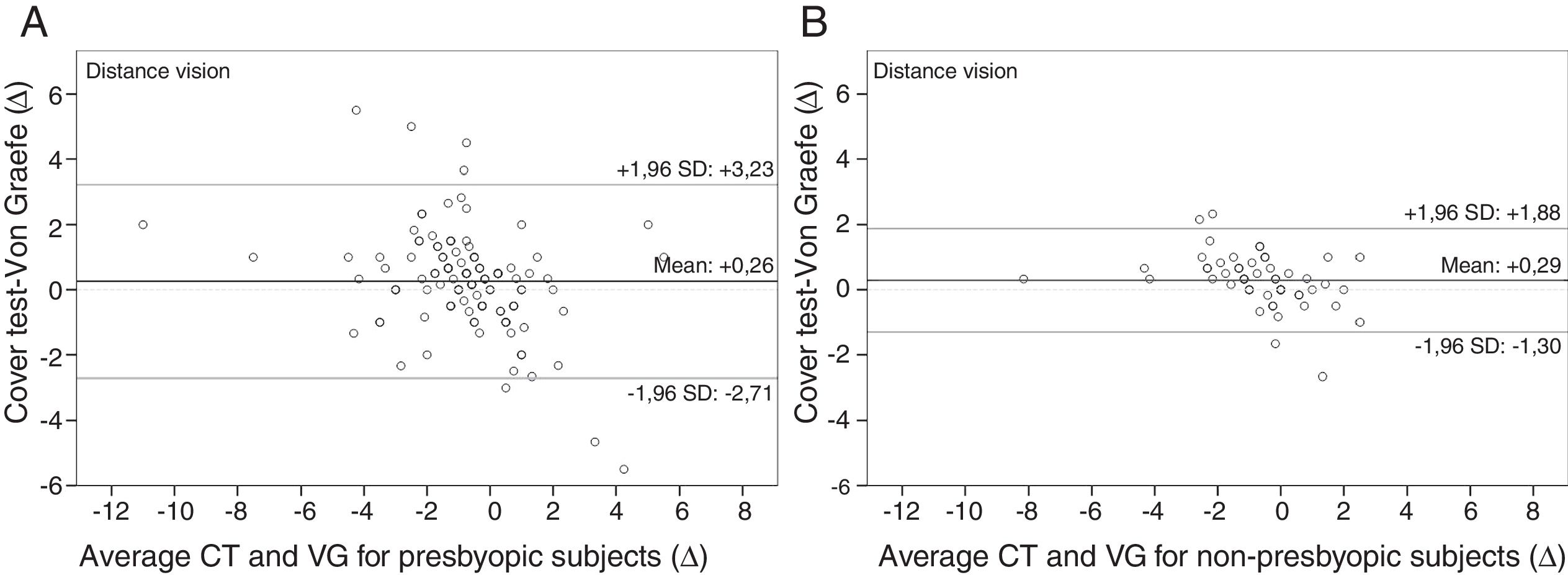
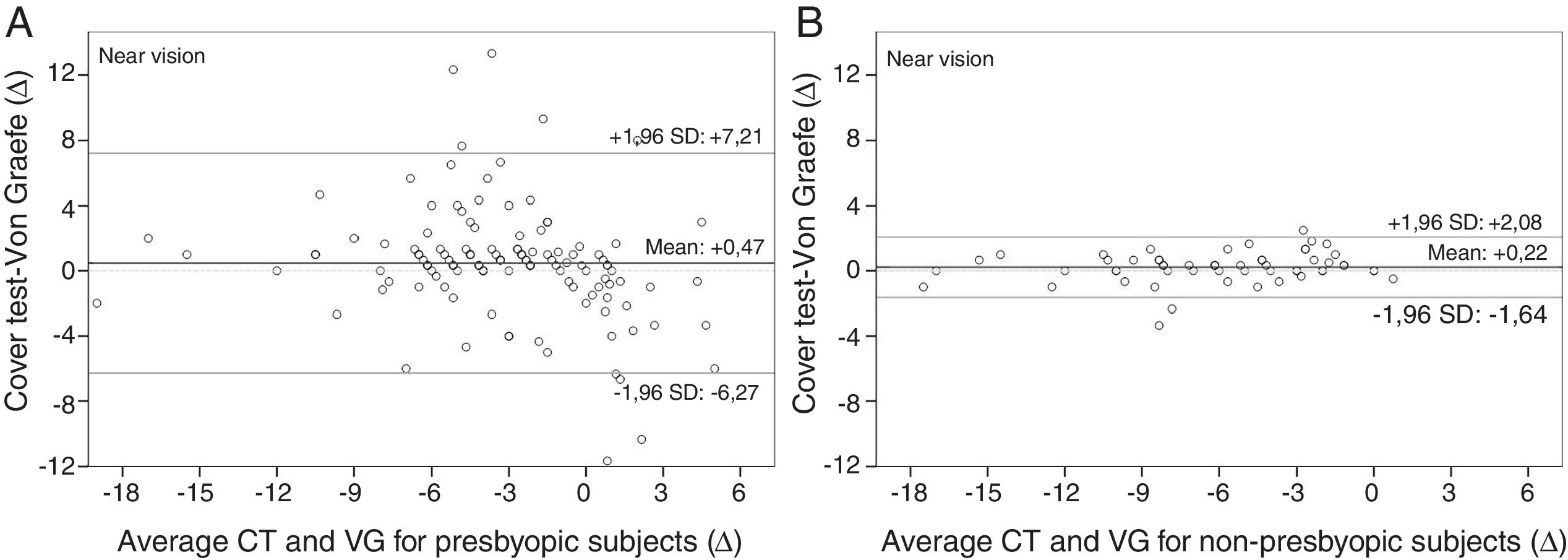
As regards the study of possible agreement between the CT and von Graefe method, Table 2 and Figs. 1 and 2 show the Bland–Altman analysis for both methods for distance and near vision. For non-presbyopic subjects, differences between the two methods for distance vision ranged over a total interval of 5.94 Δ for a given value of heterophoria, whilst the interval was even greater for near vision, at 13.48 Δ. The differences for distance vision in presbyopic subjects were located in an interval of 3.18Δ, whereas this interval was 3.72 Δ for near vision.
Agreement between cover test and von Graefe method (CT–VG) for distance and near vision.
| MD (Δ) | p | 95% CI (Δ) | CA (Δ) | 95% limits of agreement (Δ) | |
|---|---|---|---|---|---|
| Distance vision | |||||
| Non-presbyopic | +0.26 | 0.053 | −0.003/+0.53 | ±2.97 | −2.71/+3.23 |
| Presbyopic | +0.29 | 0.010* | +0.07/+0.50 | ±1.59 | −1.30/+1.88 |
| Near vision | |||||
| Non-presbyopic | +0.47 | 0.124 | −0.13/+1.08 | ±6.74 | −6.27/+7.21 |
| Presbyopic | +0.22 | 0.084 | −0.03/+0.48 | ±1.86 | −1.64/+2.08 |
MD, mean difference; CI, confidence interval for the mean difference; CA, coefficient of agreement.
The results of this research show that there are statistically significant differences between the cover test and the von Graefe method in almost all the groups analyzed, with the von Graefe method being greater than cover test and yielding more exophoric mean values than the cover test. The only group in which differences were not observed was for near vision in presbyopic subjects. In both groups of subjects and for both distance and near vision, the mean difference between both methods is less than 0.50 Δ, which results clinically insignificant. However, the coefficients of agreement indicate that both techniques for measuring the heterophoria are not interchangeable in non-presbyopic subjects. For presbyopic subjects, the coefficients of agreement are clinically acceptable, indicating that CT and von Graefe could be considered as two interchangeable methods in clinical practice.
Nevertheless, these results are not without some limitations. First, caution should be taken when extrapolating the results since the sample was not randomized and was not therefore representative. Consequently, our results should only be applied to populations presenting the same characteristics as the sample, i.e. a clinical population. Sample size also represents a limitation, since the group of presbyopic patients was not large. Statistically, this may have led to a Type II error, namely that statistically significant differences did not appear between the variables due to the small sample size.
The mean values obtained for CT and von Graefe are consistent with those offered by several authors. As an example, for distance vision and non-presbyopic subjects, Goss et al.6 obtained a mean heterophoria value of −0.2±2.6 Δ with von Graefe method, Cebrián et al.18 a value of −0.89±1.90 Δ with von Graefe, and Antona et al.17 obtained a value of −0.07±1.15 Δ with CT. For near vision and non-presbyopic subjects, the different authors establish approximately a mean value of exophoria between 3 and 4 Δ (Goss et al.6 −3.7±5.6 Δ with von Graefe, Rainey et al.3 −2.7±2.8 Δ with CT, and Sanker et al.33 −3.66±3.85 Δ with CT). These values are similar to those obtained in our study.
According to the presbyopic subjects, few studies have analyzed their heterophoria. Palomo et al.34 obtained a mean value of −0.3±2.2 Δ with von Graefe method for subjects between 51 and 70 years old and for distance vision, similar results to those showed in our study. They are not very different to those obtained for non-presbyopic subjects at distance, as it is reasonable to consider that the decreasing of accommodative amplitude should not alter the phoric status at distance vision. However, the addition prescribed for near vision does have an effect on the heterophoric value. Thus, Sheedy et al.35 found an increase of the exophoria in presbyopic subjects. Similarly, our results show a mean value of exophoria which is about twice in presbyopic subjects in comparison to the non-presbyopic group, with a similar value of standard deviation. For this reason, for presbyopic subjects the normative phoria values should move to higher values of exophoria that for non-presbyopic subjects, and this should be taken into account to assess binocular function.
In any case, our results show that there are statistically significant differences between both methods for all cases, except for presbyopic population at near vision. This finding implies that the mean values for von Graefe method are more exophoric than the CT ones. These results are consistent with those obtained by Rainey et al.,3 who also reported obtaining more exophoric values when using the von Graefe method. Moreover, there is a tendency for von Graefe results to be higher than CT ones for both esophoric and exophoric subjects. These results agree with those obtained by Calvin et al.,22 who found that the estimated cover test tended to yield lower values of heterophoria than the von Graefe method. This trend is reflected in Figs. 1 and 2, where it can be observed for non-presbyopic subjects at distance and near vision, and for presbyopic subjects it only exists for distance vision. The fact that this trend does not occur in presbyopic patients at near distance may be related to the accommodative state. The lack of accommodation causes a consistency in the measurement, resulting both methods more similar.
According to the level of agreement between CT and von Graefe, only two studies have analyzed their agreement to date,17,18 and only for non-presbyopic subjects. Our results are similar to those studies. For distance vision, Antona et al.17 obtained a CA of ±4.35 Δ, while Cebrián et al.18 found a CA of ±2.93 Δ, very similar to that obtained in our study (±2.97 Δ). At near vision, Antona et al.17 obtained a CA of ±6.54 Δ, almost equal to ours (±6.74 Δ). In all cases, these coefficients of agreement were excessively high, mainly for near vision, so that for clinical purposes it is not possible to interchange both techniques in non-presbyopic subjects. The reason for these results may be due to the repeatability of each test.18 Certainly, many studies indicate that von Graefe method is less repeatable than other techniques for measuring heterophoria in non-presbyopic subjects.3,8,10,11,17,18,20 It is not clear the reason for this high variability. One possible explanation may be the artificial environment produced by the phoropter, in addition to the length of time taken for its measurement, which may cause a change in the level of fusional vergence, altering consequently the phoria finding.3 The authors use to discard the effect of accommodation in the variability of the von Graefe test for both distance and near vision due to the use of small targets that minimize the accommodative instability.3,18 However, our results do not seem to support this idea. Results for presbyobic patients, who have diminished their accommodative ability, show that von Graefe and CT methods are interchangeable and the only factor that changes is the absence of accommodation. So, it is possible that when performing von Graefe method for non-presbyopic subjects, there may be certain instability in the accommodative system that influences in the measurement, contrary to what has been suggested to date.3,18 This is an aspect that should be studied in the future to better understand how the accommodative system may interact with the different tests that are performed when assessing the binocular function.
As far as we know, no studies specifically designed to compare both methods for presbyopic population have been reported so that comparison is difficult to discuss. In the case of presbyopic subjects, our coefficients of agreement are considerably lower than those of non-presbyopic subjects (±1.59 Δ for distance vision and ±1.86 Δ for near vision). These CA have even lower values than those considered acceptable by other authors for tests as CT and Thorington test (±2.23 Δ for distance vision18). We could therefore consider at clinical effects, that the CT and von Graefe method are two tests with a high level of agreement for both distance and near vision when considering presbyopic subjects. Our results suggest that the fact of having reduced by nature itself the accommodative ability, as it occurs in presbyopic patients, improves notably the agreement between both methods of phoria measurement. So, it seems that the absence of accommodation in presbyopic patients causes a lack of variability in the measure, being both methods more similar each other. For clinical purposes, this implies that clinicians can use any of both methods to measure the heterophoria for presbyopes, with the assurance that the value obtained is reliable with either method. This fact may facilitate the binocular vision exam in presbyopic population by simplifying the choice of the test used to assess heterophoria.
Conflicts of interestThe authors have no conflicts of interest to declare.





