






Rapid reach-to-grasp balance-recovery reactions play a critical role in preventing falls. Recent young-adult studies suggest these reactions may be guided using stored visuo-spatial information from the central field, and that peripheral vision may also play an important role. This study used gaze recordings to examine the visual control of reach-to-grasp reactions in older adults.
MethodsA motion platform was configured to simulate a “real-life” environment that included a handrail. Subjects performed an activity that required walking to the end of the platform, which was triggered to move suddenly and unexpectedly as they approached the handrail. Twelve healthy older adults (64-79 years old) were tested and compared to 12 healthy young adults (22-30 years old) tested as part of another study.
ResultsOlder adults were more than twice as likely as young adults to react to the platform perturbation by grasping the handrail (10/12 versus 4/12), despite being much less likely to visually fixate the handrail after entering the new environment. Grasping errors were remarkably common (5/10 older, 2/4 young), but there was no consistent relationship to the preceding gaze behavior.
ConclusionOlder adults were highly dependent on using a handrail to recover balance, but commonly failed to direct overt visual attention to the rail after entering the unfamiliar environment. The failure to fixate the rail required the reaching movement to be guided using peripheral vision. Further research is needed to determine whether grasping errors can be prevented via interventions that either attract overt attention to the handrail or improve processing of peripheral-field information.
Las reacciones rápidas de “alcanzar y agarrar” destinadas a recuperar el equilibrio juegan un papel fundamental a la hora de evitar caídas. Estudios recientes realizados en adultos jóvenes sugieren que estas reacciones podrían estar dirigidas por la información visuo-espacial previamente almacenada proveniente del campo visual central, y que la visión periférica podría desempeñar también un papel relevante. En este estudio se utilizaron grabaciones del recorrido de la mirada para analizar, en adultos de mayor edad, el control visual en el contexto de las reacciones de “alcanzar y agarrar”.
MétodosUna plataforma móvil se configuró de forma que simulara un entorno “de la vida real”, en el que se incluyó un pasamanos. Se pidió a los sujetos que realizaran una actividad, para la cual tenían que andar hasta el extremo de la plataforma. Dicha plataforma estaba construida de modo que se moviese bruscamente y de forma inesperada cuando el sujeto llegaba cerca del pasamanos. Doce adultos de mayor edad (64-79 años) se sometieron a esta prueba y los resultados se compararon con los obtenidos anteriormente, en el marco de otro estudio, en 12 adultos jóvenes (22-30 años). Todos los participantes gozaban de buena salud.
ResultadosEntre los adultos de mayor edad hubo el doble de casos que entre los adultos jóvenes de sujetos que reaccionaron ante la perturbación de la plataforma tratando de agarrar el pasamanos (10/12 frente a 4/12), a pesar de que hubo muchos menos sujetos de mayor edad que fijaran la mirada en el pasamanos después de entrar en el nuevo entorno. Los errores de agarre resultaron ser sorprendentemente habituales (5/10 entre los de mayor edad, 2/4 entre los jóvenes), pero no se encontró ninguna relación sistemática entre este hecho y el recorrido de la mirada anterior a la perturbación.
ConclusionesLos adultos de mayor edad resultaron depender mucho del uso del pasamanos para recuperar el equilibrio aunque, por el contrario, no dirigieron su atención visual al pasamanos una vez que entraron en el entorno desconocido. El hecho de que no fijaran la mirada en el pasamanos en ningún momento hizo que el movimiento de “tratar de alcanzar” tuviera que ser dirigido por la visión periférica. Es necesario continuar esta línea de investigación para determinar si los errores de agarre se pueden evitar mediante intervenciones que bien atraigan la atención hacia el pasamanos o que mejoren el procesado de la información proveniente de la visión periférica.
Balance-recovery reactions that involve rapidly reaching to grasp or touch an object for support are a common response to sudden “loss of balance” caused by slips, trips or other balance perturbations.1-4 These reach-to-grasp reactions are particularly prevalent in older adults and play an important role in avoiding falls.5,6 Falls in older adults are a leading cause of serious injury, loss of independence and nursing-home admission,7-9 and impose a major burden on health-care systems (e.g. 2.6 million medically-treated fall-related injuries in the United States in the year 2000, with direct medical costs of $19.2 billion).10
In order to reach to grasp or touch an object such as a handrail, the central nervous system (CNS) requires visuo-spatial information about the location of the “target”. The gaze behavior used to acquire the visuo-spatial target information needed during volitional reaching and pointing movements has been studied extensively.11 Such studies have shown that volitional arm movements performed under natural task conditions are typically guided by a saccade to the target.12 However, for compensatory reaching reactions that are triggered by sudden unexpected or unpredictable balance perturbation, the urgent need to react rapidly imposes severe temporal constraints that may limit the capacity to scan the environment for a suitable grasp target, subsequent to perturbation onset. Recent studies of young adults suggest that the CNS avoids delays in initiating rapid compensatory limb movements by utilizing previously-stored visuo-spatial information about the immediate surroundings that is automatically acquired and updated as the person moves about.13-18 It appears that this information is typically acquired via overt visual scanning and central fixation of salient objects,15,17,18 but it seems that peripheral vision may also contribute to the process.17
It is not clear whether older persons are equally able to use stored visuo-spatial information to guide compensatory reach-to-grasp reactions in the manner described above. For example, older persons may be less likely to direct attention to their surroundings (particularly when engaged in a distracting task) due to deficits in visual attention,19 or may be less able to accurately store and retrieve salient visuo-spatial information due to the decline in working spatial memory.20 Unreliable stored information could, in turn, force an increased reliance on online peripheral vision; however, the reduced spatial resolution of peripheral-field information21 could compromise reach accuracy, and age-related deficits in the ability to rapidly process information from the peripheral field could exacerbate this problem.19,22
In the present study, we explored the visual control strategies used by healthy older adults by examining their gaze behavior during reach-to-grasp reactions evoked by sudden unpredictable platform motion, using a protocol designed to simulate the heightened demands of “real-life” balance control. Thus, the platform was configured to resemble a visually-complex “real-life” living environment and subjects performed a daily-life activity that required conducting a visual search while walking to the far end of the platform. The platform was triggered to move suddenly and unexpectedly as the subject approached a handrail mounted on the platform. Subjects performed only one trial, which was their very first exposure to the perturbation and environment. Although this single-trial approach severely limits the quantity of data that can be collected, it is essential in order to avoid the adaptations that can occur when multiple trials are performed and subjects know in advance that balance perturbations may occur.23,24
The specific objective of this pilot study was to determine if there is any evidence of age-related differences in the gaze behavior used to guide the rapid reach-to-grasp reactions evoked by the unexpected perturbation while walking in the unfamiliar environment. To accomplish this, we compared data collected in older adults (as described above) to initial data from a study in which young adults performed the same protocol (King EC, et al. International Society for Posture and Gait Research 2007; Abstract MP-70), using a new data-processing methodology25 that allowed us to estimate the visual angle of the handrail for each gaze fixation. Extrapolating from previous evidence that aging may impair the ability to disengage attention from a pre-established visual target or cognitive task,26,27 we hypothesized that older adults would be less likely than younger subjects to fixate the handrail in the central visual field while ambulating in the unfamiliar environment. Such gaze behavior would be expected to increase reliance on peripheral vision to guide any attempt to grasp the rail for support in reaction to the unexpected balance perturbation. Therefore, in view of the potential difficulties in acquiring accurate information from the peripheral field,19,21,22 we further hypothesized that this gaze behavior would result in an increased likelihood of committing a motor error in attempting to grasp the rail for support.
MethodsTwelve community-dwelling older adults (6 males and 6 females; ages 64-79, height 155-190 cm, mass 44-107 kg) were tested and compared to twelve younger adults tested as part of another study, as noted above (6 males and 6 females; ages 22-30, height 154-189 cm, mass 48-127 kg). None of the subjects had participated in previous balance studies, and all were naïve to the present protocol. Volunteers were recruited via advertisements (placed in local newspapers), posters (placed in stores, churches, apartment buildings and community centers) and word of mouth, and were asked to respond (over the telephone) to questions about their medical history, mobility level and handedness. Subjects were required to be right-handed and to be able to stand and walk without aid. They were excluded from the study if they reported any: 1) neurological disorders; 2) eye disease or visual disorders; 3) vestibular or somatosensory disorders; 4) recurrent dizziness or unsteadiness; 5) use of medications that may affect balance; 6) musculoskeletal disorders or other medical conditions interfering significantly with daily activities; or 7) functional limitations of limb use. Visual acuity was tested in our laboratory, prior to starting the experiment. Subjects were required to have a minimum corrected Snellen visual acuity of 20/40 and were permitted to wear corrective lenses during the experiment. The protocol was approved by the institutional ethics review board and each subject provided written informed consent.
All of the older adults were active and independent community-dwellers. All demonstrated a high level of self-efficacy related to postural balance, with scores of 91% or above on the Activities-specific Balance Confidence (ABC) questionnaire28 (ABC scores >80% are generally associated with a high level of function and activity).29 In addition, 10 of 11 subjects reported that they engaged in 2 hours or more of strenuous (“heart beats rapidly”) or moderately strenuous physical activity at least three times per week (the 11th subject reported ≥30 minutes of mild physical activity per day; data was unavailable for the 12th subject).
The protocol was identical to that used in the earlier study involving young adults. Balance-recovery reactions were evoked by sudden, unpredictable horizontal movement of a large (2m×6m), computer-controlled, motor-driven motion platform,30,31 which was configured to simulate a realistic living environment, including a door, stair, handrail and various visual distracters (Figures 1A and 1B). A wall and door prevented the subject from viewing the environment prior to the start of the trial. A standardized script informed the subjects that there was a room behind the door, with an office area located at the far end of the room, and instructed them to open the door, enter the room, walk to the end at a normal pace and make a telephone call. This task thus required a visual search for the telephone while walking to the end of the platform. For safety, all subjects wore a harness attached (via a load cell) to a low-friction overhead track that moved smoothly and did not impede the subject's movements.
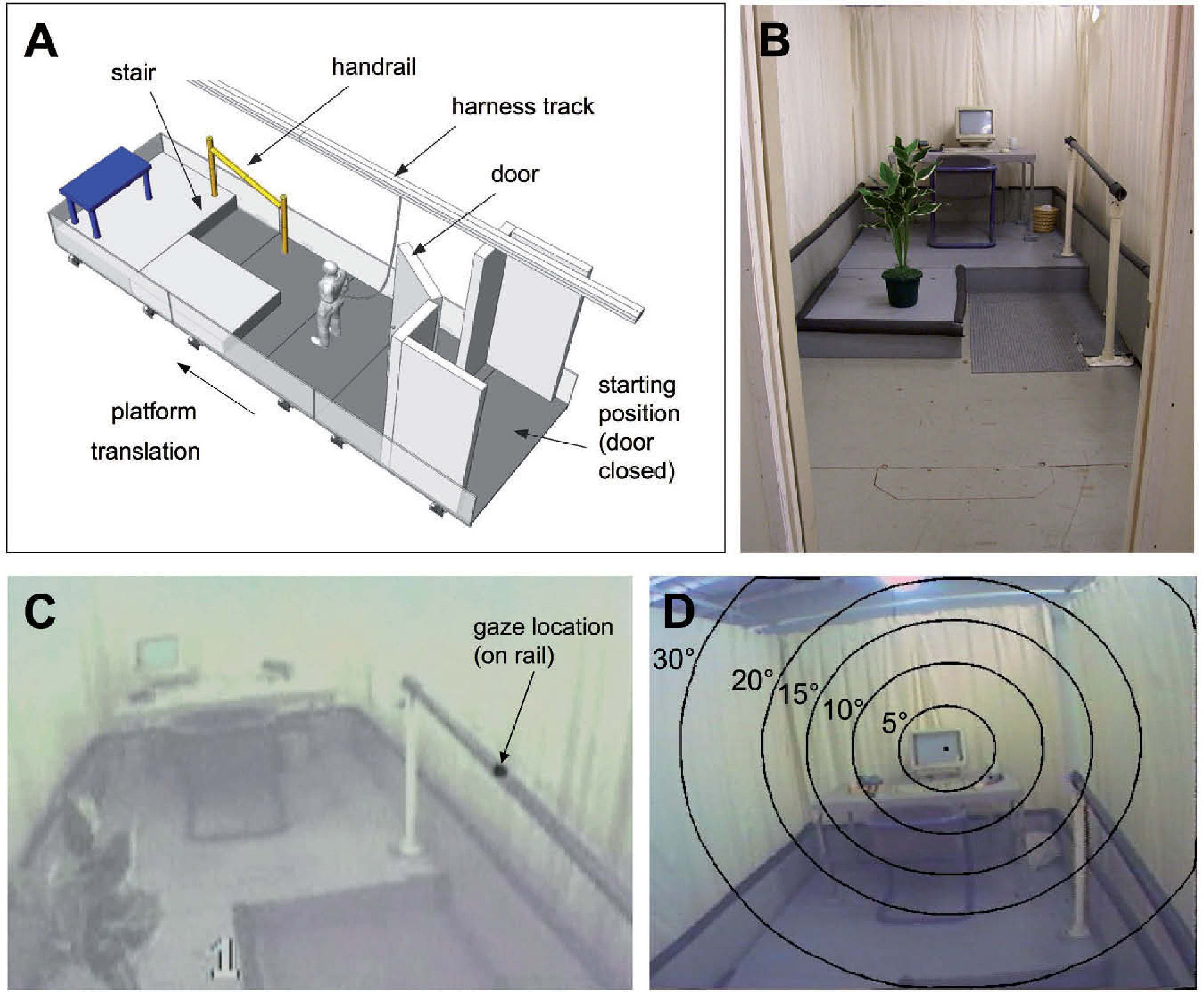
Methodological details. A. Schematic drawing of the large (6m×2m) motion platform used to evoke the reach-to-grasp reactions. B. Photograph showing the view of the platform seen by the subject after opening the door at the start of the trial (the telephone that the subject is instructed to find is located on the desk, next to the computer). C. Example video-image from the head-mounted scene-camera showing the point-of-gaze cursor superimposed by the eye-tracker software (in this example, gaze is fixated on the handrail). D. Example eye-tracker scene-camera video-image showing the point-of-gaze cursor and the superimposed “gaze ellipses” corresponding to visual angles of 5°, 10°, 15°, 20° and 30°, as calculated by the software developed by the authors25 (in the example shown, gaze is fixated on the computer screen and the far end of the handrail is visible within a visual angle of 15°).
The handrail and stair were mounted near the middle of the platform (near-end of rail 1.8 m from doorway, 1.5 m in front of stair riser). Sudden forward translation of the platform (square-wave acceleration/deceleration profile: amplitude 3.5 m/s2, peak velocity 1.1 m/s, displacement 0.43 m, duration 0.6s) was triggered to occur when the subject stepped on a pressure-sensitive mat adjacent to the handrail, thereby inducing a backward falling motion (similar to the effect of a slip). Objects mounted on the platform forced subjects to walk within a relatively narrow corridor (0.74 m wide) when approaching the stair, and thereby ensured that the handrail was well within reach when the perturbation was delivered. The rail was cylindrical, with a diameter (38 mm) and height (0.88 m above leading edge of stair tread) previously shown to allow effective grasping by persons encompassing a wide range of body heights and hand sizes.3,5,32
To avoid confounding effects of learning and adaptation, analysis was restricted to one trial per subject, which was the subject's first exposure to the platform motion and to the simulated office environment. A deception was used to ensure that the perturbation was truly unexpected: subjects were told that the first trial was a “practice trial” to help them become accustomed to the testing procedure and that the platform would not move during this trial. The effectiveness of the deception was confirmed by querying the subjects after the trial.
A three-dimensional video-based motion-analysis system (Vicon-Peak Performance, Oxford, UK) was used to determine whether the handrail was grasped or touched in reaction to the perturbation, the timing of initial rail contact and grasp completion (all fingers wrapped around the rail), and whether or not motor errors occurred. Two types of errors were identified: 1) overshoot (wrist moved laterally beyond the lateral aspect of the handrail prior to handrail contact), and 2) collision (wrist or back of the hand collided with the medial aspect of the handrail). We also determined the number of steps taken to recover equilibrium. The system comprised four cameras that provided a calibrated viewing volume (∼2m high, 2m wide, 3m long), centered near the near-end of the handrail. Coordinates of reflective markers placed on the handrail, wrist, and head were digitized (60Hz) and low-pass filtered (6Hz cut-off).
Arm-reaction onset-time was derived from surface electromyographic (EMG) recordings from the right medial-deltoid and biceps-brachii muscles (band-pass filtered, 10-500Hz; sampled at 1000Hz). EMG onset was determined by means of a computer algorithm33 and confirmed by visual inspection. All EMG, kinematic and gaze timing-values were defined relative to perturbation onset (PO) as recorded by an accelerometer (PO = platform acceleration >0.1m/s2).
A binocular head-mounted eye-tracker recorded eye movements and gaze direction (ASL model 501; Bedford, MA, USA). The eye tracker uses infrared corneal reflections to determine gaze direction, relative to the head, and superimposes the point of gaze on 60-Hz video images recorded by a forward-facing “scene camera” mounted rigidly on the head (Figure 1C). Custom-designed software25 was used to augment the point-of-gaze data, by superimposing “gaze ellipses” (corresponding to visual angles of 5°, 10°, etc, in relation to the point-of-gaze) on each frame of the scene-camera video (Figure 1D). Based on these images, central-field fixation of the handrail was deemed to have occurred if: 1) some portion of the rail was within a 5° visual angle of the point-of-gaze, and 2) this gaze location was maintained for at least 100ms.34
The primary statistical analyses involved using the non-parametric Fisher Exact Test to evaluate associations between: 1) age group and grasping behavior (number of subjects who grasped the rail in reaction to the balance perturbation); 2) age group and gaze behavior (number of subjects who fixated on the rail one or more times before or after perturbation onset); and 3) gaze behavior and overshoot/collision grasp errors. These analyses were performed using SAS statistical software (SAS Institute, Inc.; Cary, NC,USA).
ResultsOlder adults were much more likely than young adults to react to the perturbation by grasping the handrail (P=0.036): ten of twelve older subjects (83%) grasped the rail versus four of twelve young adults (25%). Of the two remaining older subjects, one leaned against the rail with the back of the forearm and the other made no overt attempt to reach for the rail. Of the eight remaining young adults, two touched the rail with the hand, three reached toward the rail but did not attempt to touch or grasp it, and three made no overt effort to reach for the rail. All touch/grasp reactions involved the right hand. No subjects touched or grasped the rail prior to perturbation onset.
The increased tendency of the older adults to use the handrail to assist in balance recovery occurred despite the fact that these subjects were less likely to direct overt visual attention toward the handrail upon opening the door and entering the new environment. Only three of twelve older adults (25%) fixated on the rail prior to perturbation onset, whereas eight of eleven young adults (73%) fixated on the rail one or more times during this interval (P=0.039; see darkened bar segments in Figure 2). [Note: this analysis was limited to eleven young adults due to technical problems with the gaze data in the 12th young subject.]
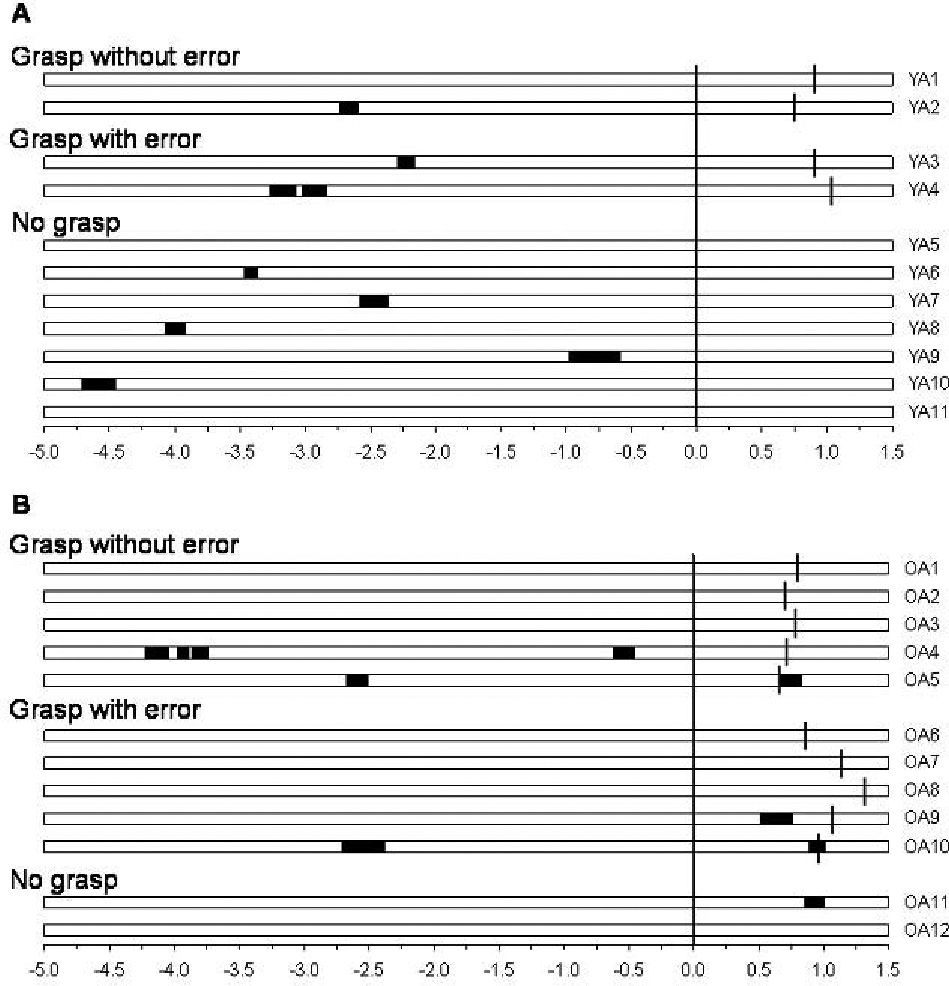
Visual fixation of the handrail displayed as a function of time, in the young adults (A) and older adults (B). Time-zero corresponds to the onset of the balance perturbation (platform acceleration >0.1m/s2); negative and positive time values (in seconds) correspond to events occurring before and after the perturbation onset, respectively. Each of the 23 horizontal bars corresponds to the trial performed by one of the 11 young adults for whom gaze data were available (subject numbers YA1, YA2, etc) or one of the 12 older adults (subject numbers OA1, OA2, etc). Each darkened portion of the bar represents an interval during which gaze was fixated on the handrail (within a visual angle of 5°). The vertical line segments superimposed on the bars (in grasping trials) indicate the time at which the grasp was completed (fingers fully wrapped around the rail). Note the greater tendency for the young adults to fixate on the rail prior to perturbation onset, and for the older adults to fixate on the rail after perturbation onset.
All of the reach-to-grasp movements, in both age groups, were initiated in the absence of a concomitant saccade to the handrail (see Figure 3 for illustrative data). In fact, in all but two cases, there was no visual fixation of the rail at any time during the interval from perturbation onset to grasp completion (see Table 1). Two older adults (subjects OA9 and OA10 in Table 1) did fixate on the rail during this time interval; however, these fixations occurred more than 250ms after the initiation of the arm reaction (as defined by the earliest activation in biceps or deltoid). Both of these trials involved overshoot errors, and the timing of the fixation appeared to be associated with a relatively late adjustment to the reaching movement, occurring just prior to (OA9) or during (OA10) the corrective reversal in the wrist trajectory (see Figure 3B).
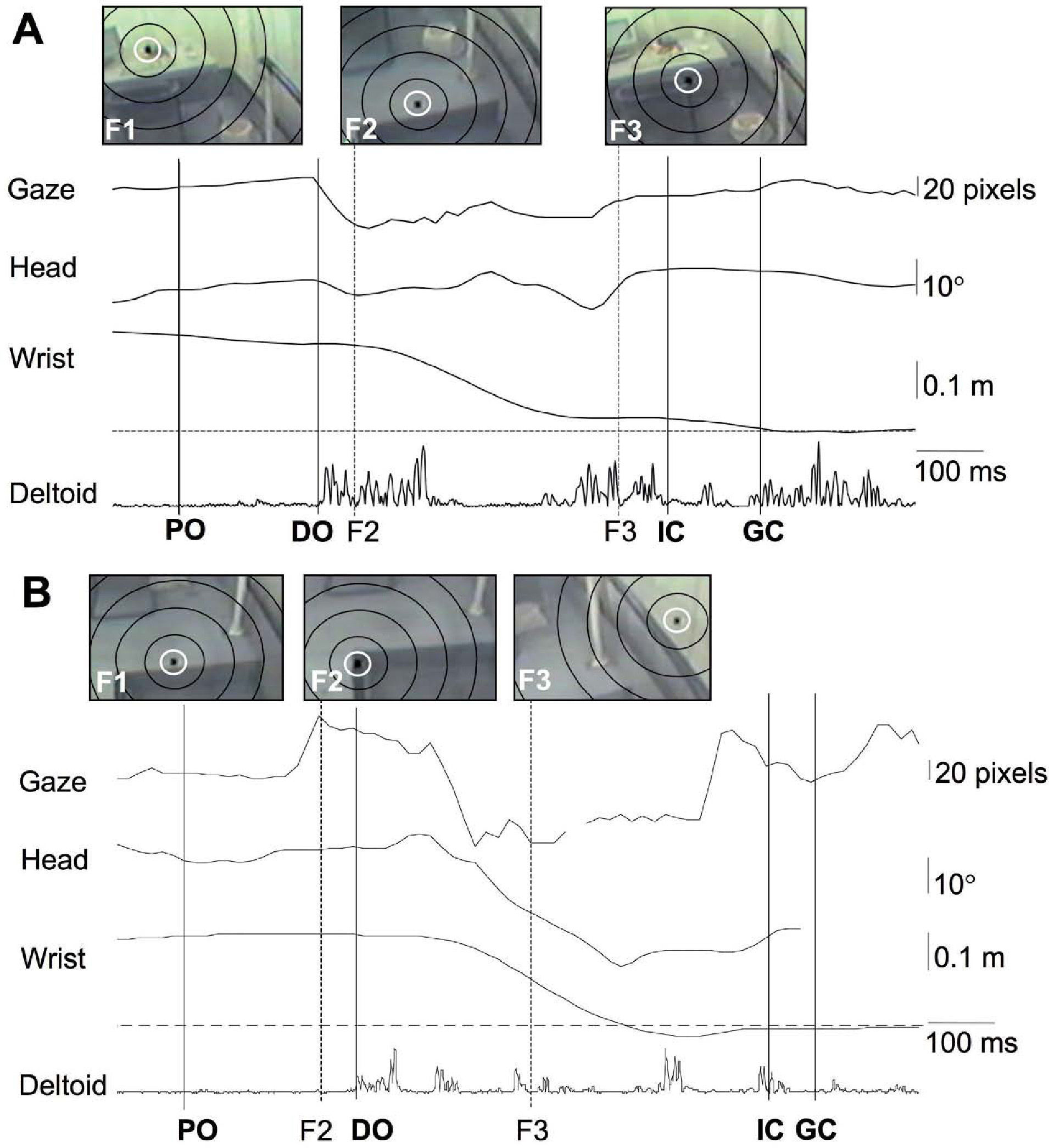
Recorded data for the case of a young-adult (A) and an older-adult (B) trials. In A (subject YA1), the handrail was grasped without overt error, whereas the hand initially overshot the rail in B (subject OA9). Each panel displays horizontal eye movement (relative to the head), transverse-plane head rotation, lateral wrist displacement (relative to the handrail) and rectified EMG from the right medial-deltoid muscle. Downward displacements indicate lateral motion. The vertical lines indicate time of perturbation onset (PO), onset of deltoid activation (DO), initial contact with the rail (IC), grasp completion (GC), and the onset of each visual fixation occurring after PO (F2, F3). The broken horizontal line indicates the location of the handrail in relation to the wrist marker. The inset images from the eye-tracker scene-camera show the point of gaze (black square symbol within a white circle) at the onset of the indicated post-PO visual fixations (F2, F3), as well as the fixation in effect at time of PO (F1); the black ellipses indicate visual angles of 5°, 10°, 15° and 20° with respect to the point of gaze. These images clearly indicate that the arm reaction was initiated in the absence of any direct fixation of the handrail (i.e. visual angle always >5°). Although there was an early post-PO saccade (F2) in both A and B, this saccade was not directed at the handrail and did not result in central fixation of the rail (visual angle >20°). A central fixation of the rail (visual angle <5°) did occur in B (F3), but this was much later in the response (>250 ms after the initiation of the arm reaction).
Summary of the grasping reactions and the associated gaze behavior (central-field fixations of the handrail are highlighted in bold text)
| Subject | Grasp reactions | Gaze fixations§ | |||||||||
| Grasp error | Timing (ms)¶ | Prior to perturbation onset¥ | At perturbation onset | After perturbation onset† | |||||||
| EMG onset | Grasp com-plete | Target | Visual angle to rail | End time (ms)¶ | Target | Visual angle to rail | Target | Visual angle to rail | Onset time (ms)¶ | ||
| Young adults: | |||||||||||
| YA1 | --- | 94b | 873 | phone | 10-15° | -977 | phone | 15-20° | stair | 20-30° | 257 |
| chair | 15- | 640 | |||||||||
| YA2 | --- | 166 | 718 | rail | 0-5° | -2598 | phone | 10-15° | --- | --- | --- |
| YA3 | collision | 196 | 873 | rail | 0-5° | -2160 | chair | 15-20° | chair | 15-20° | 857 |
| YA4 | overshoot | 185 | 998 | rail | 0-5° | -2835 | phone | 10-15° | post | 5-10° | 748 |
| phone | 10-15° | 898 | |||||||||
| Older adults: | |||||||||||
| OA1 | --- | 313 | 772 | phone | 10-15° | 105 | phone | 10-15° | --- | --- | --- |
| OA2 | --- | 242 | 683 | chair | 10-15° | -1883 | floor | 20-30° | --- | --- | --- |
| OA3 | --- | 250 | 755 | chair | 5-10° | -1278 | chair | 15-20° | phone | 15-20° | 105 |
| OA4 | --- | 230b | 692 | rail | 0-5° | -458 | stair | 15-20° | post | 5-10° | 492 |
| OA5 | --- | 307 | 643 | rail | 0-5° | -2507 | phone | 15-20° | post | 5-10° | 477 |
| OA6 | collision | 231 | 838 | post | 5-10° | -4078 | stair | 20-30° | --- | --- | --- |
| OA7 | collision | n/a£ | 1117 | chair | 5-10° | -2200 | stair | 20-30° | --- | --- | --- |
| OA8 | overshoot | 271 | 1305 | phone | 5-10° | -1028 | desk | 10-15° | stair | 10-15° | 488 |
| chair | 20-30° | 1205 | |||||||||
| OA9 | overshoot | 253 | 945 | desk | 5-10° | -2488 | stair | 15-20° | stair | 20-30° | 212 |
| rail | 0-5° | 512 | |||||||||
| OA10 | overshoot | 288b | 940 | rail | 0-5° | -2377 | floor | 20-30° | rail | 0-5° | 890 |
See Figure 1B for a photograph showing the location of the various fixation targets noted in the table (“post” indicates the far post of the handrail).
All timing values are in relation to perturbation onset (time=0.0); negative values indicate events occurring prior to perturbation onset.
For the pre-perturbation fixations, the displayed data correspond to the nearest fixation (smallest visual angle) with respect to the handrail.
Grasping errors were remarkably common in both age groups. Five of the ten older adults who grasped the handrail in reaction to the perturbation exhibited clearly-visible motor errors during the movement of the hand toward the rail (three overshoot and two collision errors), and two of the four young adults who grasped the rail also made such errors (one overshoot, one collision). In all cases, subsequent corrective arm movements eventually resulted in a successful grasp of the rail, and all subjects were able to recover equilibrium without relying on the safety harness for support (peak harness loading <12% of body weight in all trials). The grasping reactions were always accompanied by one or more compensatory (stabilizing) steps, and there appeared to be a tendency for more steps to be required in trials involving a grasping error (median number of compensatory steps: 3.3 in error-trials vs. 2.4 in no-error trials). Ad hoc analysis, however, failed to demonstrate a statistically significant association between grasp errors and number of compensatory steps (one-sided Wilcoxon test, P=0.09).
There were no consistent links between the occurrence of grasping errors and the prior gaze behavior. Among the 14 subjects (10 older, 4 young) who grasped the handrail, overshoot or collision errors were equally likely to occur whether or not the subject looked at the rail prior to perturbation onset (P=1.00). In contrast, there did appear to be some evidence of a trend within the older adults: grasp errors occurred in only one of the three subjects who fixated on the rail prior to perturbation onset (33%), whereas such errors occurred in four of the seven subjects (57%) who failed to look at the rail prior to the perturbation. However, among the four young adults who grasped the rail, two of the three subjects who fixated the rail prior to the perturbation subsequently committed grasp errors, whereas the one subject who did not look at the rail was able to grasp it without overt error.
DiscussionThe results of this pilot study support the hypothesis that older adults would be less likely than younger subjects to look at a handrail as they entered and walked through an unfamiliar environment. The failure to fixate the rail required the subsequent reach-to-grasp balance-recovery reactions to be guided using peripheral vision. It is well known that the peripheral visual field provides lower spatial acuity than the central field,21 and studies of volitional arm movements have demonstrated that a forced reliance on peripheral vision leads to reduced accuracy in pointing or reaching toward a target.35-41 Furthermore, aging commonly impairs the ability to detect and process peripheral information.19,22 We had therefore hypothesized that older subjects who failed to look at the rail prior to the perturbation would be more likely to commit errors during the subsequent perturbation-evoked reaching reaction. The initial data presented here did suggest some trends that are consistent with this hypothesis (i.e. grasping errors in four of the seven older adults who failed to look at the rail); however, a larger sample will be required to ascertain statistical significance.
Impaired ability to grasp the rail effectively is likely to be dependent on a number of factors related to vision and the processing of visual information, as well as on other (non-visual) neuro-musculoskeletal factors. Although the cohort was screened to exclude subjects with diagnosed visual, neural or musculoskeletal disorders and all subjects appeared to be healthy and active, it is quite likely that individual subjects had varying degrees of sub-clinical deficits related to the effects of normal aging.42 In addition, some subjects may have been more confident or experienced in moving about in unfamiliar environments, as a consequence of greater exposure to this type of activity in their daily lives. These sources of inter-subject variability may explain why we were unable to establish a strong relationship between the gaze behavior and the accuracy of the subsequent reach-to-grasp reactions in our cohort. In daily life, there are additional environmental factors (e.g. low levels of ambient illumination, low contrast between handrail and background, glare) that may exacerbate age-related visual deficits, and thereby elevate the importance of adopting gaze behavior that will provide the best possible visuo-spatial information for guiding reach-to-grasp reactions. Direct visual fixation of the rail would be expected to provide the best possible visuo-spatial information; however, the findings of the present study indicate that older adults are less likely than younger persons to exhibit such gaze behavior, and suggest that this factor may possibly impede the ability of some individuals to grasp the rail effectively, even when environmental lighting conditions are good. Work in progress is directed at verifying these results in a larger cohort and identifying the specific aspects of gaze behavior and visual processing that best predict impaired grasping reactions (McKay SM, et al. International Society for Posture and Gait Research 2007; Abstract SP-14).
The present study also demonstrated that older adults were more likely than the young to rely on using a handrail to recover balance. Although this has also been observed in previous studies,43-45 the present study is (to our knowledge) the first to show that this increased reliance on handrails occurs even when the perturbation is truly unexpected, and is not simply a pre-planned strategy to safeguard stability during a forthcoming (anticipated) perturbation. In addition, the present findings regarding the prevalence of motor errors during the arm reactions extend previous reports of age-related impairments related to slowing of the arm reactions.5,6 In the present study, subjects were apparently able to compensate for any instability arising from the grasping errors by executing compensatory steps; however, a reliance on stepping to recover balance may be problematic for individuals who are unable to execute stepping reactions effectively (as is the case for many older adults),5,6 or in situations where environmental features (e.g. clutter on floor, furniture, curbs, stairs) may limit the capacity to recover balance by stepping.
The failure of many of the older adults to look at the handrail prior to the perturbation could possibly reflect difficulty in disengaging visual attention from the ongoing (“telephone”) task.46 It is also possible that the failure to scan the environment as thoroughly as the young adults could reflect a strategy of minimizing head and eye motion during ambulation, so as to avoid instability that can be induced by eye and head movements47 and to optimize the visual and vestibular feedback needed to keep the body upright.48 Further research is needed to examine these possibilities.
In summary, the present study has provided new information regarding age-related deficits in the capacity to automatically scan the surroundings and redirect central vision so as to detect salient objects, such as handrails, while moving about in an unfamiliar environment. Previous studies would suggest that the capacity of older adults to derive such information from the peripheral visual field is also impaired.19,22 Taken together, such findings suggest that interventions that either attract overt attention to the rail (central fixation) or improve ability to process covert visual information (from the peripheral visual field) may reduce the incidence of grasping errors in older adults and thereby help to reduce risk of falling. We are currently working toward this objective, via the development and testing of handrail cueing systems18,30,31,49 and “visual training” programs.18
Financial disclosure: None of the authors have a commercial or financial interest in the methods, devices or procedures mentioned in the study. This study was funded by operating grant #MOP-13355 from the Canadian Institutes of Health Research (CIHR). S.M.M. held a summer internship award from the Ontario Neurotrauma Foundation and a CIHR Strategic Training Post-Doctoral Fellowship in Health Care, Technology and Place. E.C.K. held scholarships from the CIHR, the Toronto Rehabilitation Institute, and the University of Toronto (Institute of Biomaterials and Biomedical Engineering, and Vision Science Research Program). The authors would like to thank Areeba Adnan, Rachel Keshwah and Aaron Marquis for their assistance with this study. Results were presented in preliminary form at the 18th Conference of the International Society for Posture and Gait Research held in Burlington, Vermont, USA in July, 2007 (Lee TA, Scovil CY, McKay SM, Peters AL, Maki BE. Age-related differences in reach-to-grasp reactions and associated gaze behavior evoked by unexpected perturbation when walking in an unfamiliar environment).





