








The aim of this pilot study was to test whether retinitis pigmentosa patients would benefit from filter contact lenses as an effective optical aid against glare and photophobia.
MethodsFifteen subjects with retinitis pigmentosa were enrolled in this study. All of them were evaluated with filter soft contact lenses (MaxSight), filter glasses (CPF 527) and without filters (control). All patients were assessed for the three aid conditions by means of best corrected visual acuity (BCVA), contrast sensitivity (without glare and with central and peripheral glare)(CSV-1000) and a specific subjective questionnaire about quality of vision.
ResultsBCVA was slightly better with filters than without filter but the differences were not statistically significant. Contrast sensitivity without glare improved significantly with the contact lenses (p<0.05). The central glare had significant differences for the frequencies of 3 cpd and 18 cpd between the contact lens filter and the control group (p=0.021 and p=0.044, respectively). For the peripheral glare contrast sensitivity improved with contact lens versus control group for highest frequencies, 12 and 18 cpd (p<0.001 and p=0.045, respectively). According to the questionnaire the contact lens filter gave them more visual comfort than the glasses filter under the scenarios of indoors glare, outdoors activities and indoors comfort.
ConclusionThe filter contact lenses seem to be a good option to improve the quality of vision of patients with retinitis pigmentosa.
El objetivo de este estudio preliminar fue comprobar si los pacientes con retinitis pigmentosa se beneficiarían de lentes de contacto con filtro como ayuda óptica eficaz contra el deslumbramiento y la fotofobia.
MétodosEn este estudio se incluyeron 15 sujetos con retinitis pigmentosa. Todos fueron evaluados con lentes de contacto blandas con filtro (MaxSight), gafas con filtro (CPF 527) y sin filtro (control). En todos los pacientes se evaluaron los tres medios de apoyo basándose en la agudeza visual con mejor compensación (AVMC), la sensibilidad al contraste (sin deslumbramiento y con des lumbramiento central y periférico) (CSV-1000) y un cuestionario subjetivo específico sobre la calidad de la visión.
ResultadosLa AVMC fue ligeramente mejor con filtro que sin filtro, aunque las diferencias no fueron estadísticamente significativas. La sensibilidad al contraste sin deslumbramiento mejoró de manera significativa con las lentes de contacto (p<0,05). El deslumbramiento central presentó diferencias significativas para las frecuencias de 3 cpd y 18 cpd entre las lentes de contacto con filtro y el grupo de control (p=0,021 y p=0,044, respectivamente).
En cuanto al deslumbramiento periférico, la sensibilidad al contraste mejoró con las lentes de contacto frente al grupo de control para las frecuencias más altas, 12 y 18 cpd (p<0,001 y p=0,045, respectivamente). Según el cuestionario, las lentes de contacto con filtro les proporcionaron más confort visual que las gafas con filtro para situaciones de deslumbramientos en interiores, actividades al aire libre y confort en interiores.
ConclusionesLas lentes de contacto con filtro parecen una buena opción para mejorar la calidad de la visión de los pacientes con retinitis pigmentosa.
Retinitis pigmentosa is a bilateral retinal hereditary dystrophy. The most common symptoms for this disease are nyctalopia and poor dark adaptation, difficulty with orientation and mobility, reduced central visual acuity and blue-yellow channel dyschromatopsis.1–6 Previous studies show that this condition ranks fifth among all hereditary diseases and it is the fourth most frequent cause of severe visual disability with a prevalence of 1 for every 5000 inhabitants.4,5 In Spain, one in every 80 people carry the affected gene and in total there are 15,000 patients affected by this disease.7 Retinal pigmentosis is a hereditary transmitted disease that is gender-linked and that can be recessive autosomic or dominant autosomic.8,9
Today the term retinitis pigmentosa includes a wide spectrum of disorders with chromosomal findings, most commonly associated with a progressive degeneration of the visual photoreceptors.2,10,11
Selected wavelength filters are used for protecting the retina and other ocular tissue against sunlight, making a very valuable contribution to low vision rehabilitation for retinitis pigmentosa patients.12,13 They improve the quality of vision by reducing the recovery time of changes in light adaptation. They decrease light dispersion inside the ocular media and the chromatic aberration, with the subsequent increase of the contrast of the retinal image.14
The most commonly used filters used by retinitis pigmentosa patients are those absorbing wavelengths below 550nm.14 These lenses have an orange tonality that despite the initial refusal by the patients on a first trial, are nevertheless of great help for them to reduce the night blindness difficulties, glare and contrast sensitivity on light-to-darkness changes of illumination.
Rosemblum et al12 observed that orange filters (550nm) decrease photophobia by selecting the retinal rods. These filters also decrease the chromatic aberration and, consequently, increase image contrast in the retina. They also observed that most of the CPF-550 filter wearers had their glare sensitivity improved. López-Alemany and Uson15 in 2007 proposed tinted contact lenses as a potential aid to help some cases of low vision patients that would need filters that absorb specific wavelengths. Hydrogels are good materials to tint and this peculiarity eases the fabrication of customized filters that might be needed for every patient.
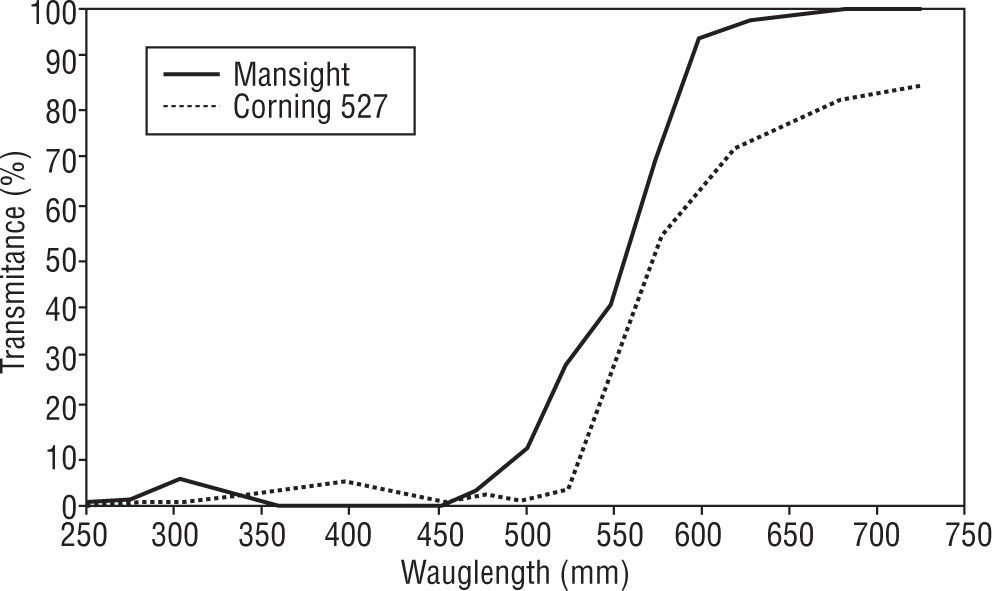
The MaxSight® Amber contact lens was commercialized by both the companies Nike and Bausch&Lomb laboratory. It has an absorption curve comparable to a CPF527 filter that increases the contrast and protects from ultraviolet A and B light when exercising outdoors. Figure 1 shows the transmission curves for the two filters for easy comparison. Although these contact lenses were not originally designed to be a low vision aid they could be useful for retinitis pigmentosa patients as they have a red filter that only transmits 10% of the wavelengths below 500nm. The use of these contact lenses would avoid peripheral light entering the eye from the side of the glasses and also eliminate the reflections on the interior surface of the lens.10 Furthermore, the use of a contact lens represents an esthetic improvement over glasses.
The aim of this pilot study was to test if retinitis pigmentosa patients would benefit from contact lenses filters as an efficient optical aid against glare and photophobia. With this aim, patients were provided with the filter on glasses and contact lenses to try for a week each and test if they improve visual comfort.
Material and methodsPatientsThe study was conducted in compliance with good clinical practice guidelines, institutional review board regulations and the tenets of the Declaration of Helsinki. All patients were given a written explanation of the study and then signed a consent form. This consent form explained that the enrolment in this study did not imply any risk to their health and that they had the right to withdraw from the study at any time. The aim of the study was masked for examiners. All patients had been diagnosed of retinitis pigmentosa and they were members of the Asociacion Retina Madrid. The inclusion criteria were: 1) a maximum refractive error of 3 diopters in best sphere with a maximum astigmatism of 0.75 diopters. 2) Patients also had to be free from cataract, dry eye pathology or any other condition affecting the ocular surface that would make the patient unsuitable for contact lens wear.
Clinical testsAll patients went through an eye test to determine the required refraction for both the contact lens and glasses with filter. They had their distance best corrected visual acuity (BCVA) measured by means of Snellen charts and recorded in LogMAR units.
Contrast sensitivity was tested with and without glare taking into account that glare could be central or peripheral. The CSV-1000 (Vector-Vision, Dayton, Ohio, USA) was used. It has proved to be clinically repeatable and useful for monitoring changes in contrast sensitivity.16 This test has a translucid retroilluminated panel of 85cd/m2 and was performed in a room with a luminance of 90 lux. Contrast sensitivity was tested at four spatial frequencies (3, 6, 12 and 18 cpd) by means of a 2-AFC (2 alternative forced choice). To test the glare contrast sensitivity a lamp of 200 lux was placed behind the patient so that its light would reflect on a mirror and towards the patient's head.17 Both frontal and peripheral glare were then tested. For the frontal glare the mirror was right above the CSV-1000 test and to simulate the peripheral glare the mirror was placed at 1.5 meter distance to the right of the test chart.
Patients then had a slit lamp examination to determine whether they were free from cataract and therefore suitable for the study. They were then shown and tried the glasses and contact lens filters. The glasses filters used in this study were the CSF-Corning 527 (AVS Baja Vision S.A, Madrid, Spain) for being one of the most used filters among patients suffering from retinitis pigmentosa.13 This filter has a transmission that varies between 32% on the lightened state and 11% on the darkened state. THE contact lens filter patients were fitted the MaxSight Amber (B&L, Rochester, USA). This is a hydrophilic contact lens that was designed for performing outside sports because it filters 80% of the light bellow 527nm. This contact lens is made of Polymacon and has a spherical front surface, a diameter of 14mm and a Dk of 54 and has a range of prescribed powers of +6.00 to −9.00 with 0.25 D steps.
All the previously mentioned tests were performed during the first visit. Patients left with a pair of glasses equipped with the CSF-Corning 527 filter or a MaxSight Amber pair of contact lenses. The distribution of patients into these two groups was random. Half of the study patients were asked to wear the glasses filter for the following week and the other half to wear the contact lens filter. They were instructed to wear the filters every day and for a minimum of 8 hours. Patients then attended a first follow-up visit one week later. On this visit, visual acuity, contrast sensitivity and slit lamp examination were performed.
Finally, they attended a second follow-up visit that was one week after the first follow-up. During this second week patients had been asked to swap their glasses for contact lens filter or vice versa according to the group they belonged to. In addition to visual acuity and contrast sensitivity, in this visit, they were asked to fill in a questionnaire that was specially designed for the study. This subjective test was made up of 4 items where patients had to decide whether the activities of daily living mentioned on the items were easier to perform with the filter on contact lenses, glasses or neither of them (see table 1).
Statistical analysisAll analysis were carried out using SPSS, version 15 for Windows (SPSS, Inc., Chicago, IL). The values shown on the results section are the means ± SD for the experiments performed. Normal distribution of variables was assessed by the Kolgomorov-Smirnov normality test. Parametric test were used to compare the studied groups. Differences between glasses, contact lenses and non-filters values (control) were estimated based on the Student t test for matched-pairs with p-values. P<0.05 being deemed as statistically significant.
ResultsPatientsFifteen patients, 4 females and 11 males, took voluntary part in the present study with a mean age of 51.47±5.15 (range 45 to 60). Their mean refractive sphere and cylinder were−2.34±0.53D (range −1.25, −3.00) and −0.39±0.28 (range 0, −0.75), respectively. None of the patients that took part on the study had any difficulties adapting to wear contact lenses. However, one of them had difficulties with the handling of the contact lens and needed help for insertion and removal.
Visual acuitiesThe BCVA were 0.23±0.08 LogMAR for the no-filter condition, 0.19±0.06 LogMAR for the contact lens filter and 0.19±0.07 LogMAR for the glasses filter. Although the BCVA was slightly better with any of the filters than with no filter the differences were not statistically significant (p=0.133 and p=0.156 respectively).
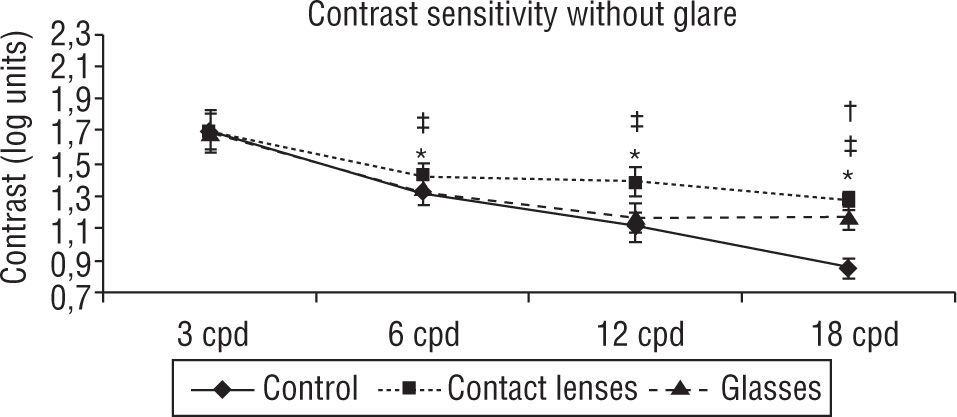
Contrast sensitivity and glareTable 2 contains all contrast sensitivity scores. The Contrast sensitivity without glare improved significantly with the contact lens filter in comparison to not using a filter or to using the glasses filter. This difference was statistically significant for all frequencies (p<0.05) apart from the 3 cpd one. There were no significant differences between not using a filter and using the glasses filter with the exception of the highest frequency (p<0.005) (see figure 2).
Contrast sensitivity scores (Mean + SD and p values for the significant cases)
| Control | Contact lenses | Glasses | |
| Contrast sensitivity without glare | |||
| 3 cpd | 1.71±0.12 | 1.70±0.11 | 1.69±0.12 |
| 6 cpd | 1.34±0.10a (p=0.036) | 1.42±0.09b (p=0.019) | 1.34±0.09 |
| 12 cpd | 1.11±0.09a (p<0.001) | 1.39±0.09b (p<0.001) | 1.17±0.09 |
| 18 cpd | 0.86±0.06a (p<0.001) | 1.28±0.04b (p<0.001) | 1.18±0.08c (p<0.001) |
| Contrast sensitivity with central glare | |||
| 3 cpd | 1.48±0.12a (p=0.021) | 1.61±0.17 | 1.63±0.09c (p=0.001) |
| 6 cpd | 1.26±0.08 | 1.33±0.11 | 1.37±0.12c (p=0.005) |
| 12 cpd | 1.18±0.09 | 1.17±0.09 | 1.18±0.08 |
| 18 cpd | 1.04±0.07a (p=0.044) | 1.09±0.10 | 1.09±0.08c (p=0.041) |
| Contrast sensitivity with peripheric glare | |||
| 3 cpd | 1.63±0.13 | 1.67±0.11 | 1.59±0.15 |
| 6 cpd | 1.40±0.13 | 1.33±0.12 | 1.41±0.10 |
| 12 cpd | 1.04±0.09a (p=0.045) | 1.09±0.08 | 1.09±0.07c (p=0.043) |
| 18 cpd | 1.00±0.06a (p<0.001) | 1.11±0.07 | 1.13±0.08c (p<0.001) |
For the central glare readings of contrast sensitivity there were significant differences for the frequency of 3 cpd and 18 cpd between the contact lens filter and the control group (p<0.05). For the results using the glasses filter there was a significant improvement for the two lowest spatial frequencies and 18 cpd frequency when compared to the control group (p<0.05) (see figure 3).
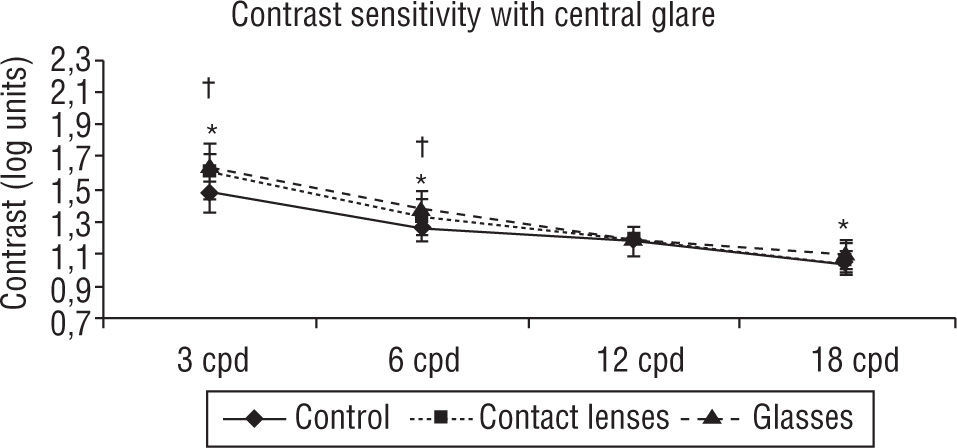
Contrast sensitivity with central glare. Significant differences for the frequency of 3 cpd between the contact lens filter and the control group and glasses filter with control (p<0.05). Also, between the glasses filter and control there was a significant improvement for 6 cpd spatial frequency (p<0.05). Student-t test for matched-pairs. *p<0.05 Control vs. Contact lenses; ‡p<0.05 Contact lenses vs. Glasses; †p<0.05 Control vs. Glasses.
Finally, the peripheral glare readings of contrast sensitivity showed the smallest differences between the three groups. The glasses filter and contact lens improved with respect to control for the two highest frequencies, 12 cpd and 18 cpd (p<0.05) (see figure 4).
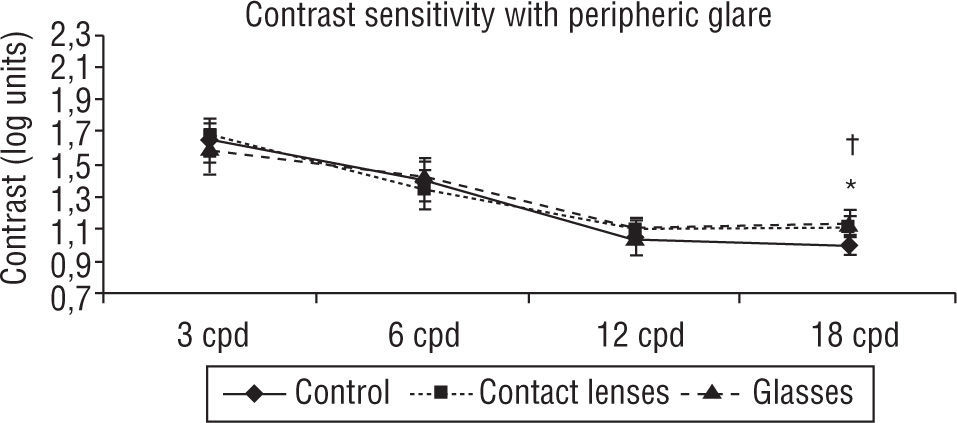
Contrast sensitivity with peripheric glare. The glasses filter and contact lens improved with respect to control for the highest frequency, 18 cpd (p<0.05). Student-t test for matched-pairs. *p<0.05 Control vs. Contact lenses; ‡p<0.05 Contact lenses vs. Glasses; †p<0.05 Control vs. Glasses.
The data collected from the questionnaires show a preference for the contact lens filters for most conditions (see table 1). The largest comfort was obtained when wearing the contact lens filter with respect to the glasses filter under conditions of indoor glare, outdoor activities or indoor comfort. The two filters showed no significant difference regarding color perception. Our results show that 77.7% of the patients would benefit from alternating between the glasses and filters contact lens or even replace the glasses by contact lenses. The remaining 22.3% would prefer glasses over contact lenses.
DiscussionThe results from this pilot study show a significant improvement on the quality of contrast vision of patients with retinitis pigmentosa when wearing the filters on contact lenses or glasses in comparison to control. Red filters could be helpful to patients suffering from retinitis pigmentosa for improving contrast sensitivity, visual acuity, although, there is a little evidence to indicate that filters improve visual skills.12,18,19 Nevertheless, filters diminish short wavelength exposure, minimizing photoreceptor damage.12,20 The potential benefits of these filters in contact lenses for patients with retinitis pigmentosa has only been investigated in Bothnia dystrophy, a variant of retinitis pigmentosa which affects the visual cycle. In this study, patients with Bothnia dystrophy vision and comfort were improved by dark brown tinted contact lenses.21
When patients with retinitis pigmentosa wore the filters on contact lenses they gave a significant improvement in contrast sensitivity in comparison to wearing them on glasses. The contrast sensitivity without glare improved with the use of filters on contact lenses with respect to glasses. It has been reported that retinitis pigmentosa patients can experience glare by physical factors, such as AN inappropriately placed light source.22 In this case improvement, could be due to the contact lenses filtering all the light coming into the retina whilst with glasses some lateral light is expected to enter the eye without being filtered and thus disperses into the eye.13 Or perhaps it is the fact that glasses are more prone to suffer from internal reflections on the lenses than a contact lens, particularly when they are indoors under artificial lights.
Patients filled a questionnaire at the end of the study. The aim was to obtain information about the preferences of the patient to compare both filters, and for this reason, there has been no statistics performed for these results. One of the most common complaints among patients using the filters on glasses related to indoors activities as the filters decrease the luminosity and therefore the visibility of the objects.13 Up to now these filters have only been prescribed on glasses. However, yellow filters have proven to be helpful in intraocular lenses13,15,23 and it could be that red filters might be of more benefit when worn on contact lenses than on glasses.15 Two thirds of the patients were more comfortable with the contact lens than the glasses filter for indoor use. This could be due by the fact that retinitis pigmentosa patients have difficulty adapting to even small changes in light levels24 and probably wearing contact lens filter provides a constant dark adaptation, diminishing symptoms of light sensitivity in the retina.
Before patients could benefit from this contact lens filter we would need to overcome two lens limitations. The first one is that this lens is discontinued from the market and therefore nowadays not a treatment option for patients with retinitis pigmentosa. This reduces the clinical significance of this study but on the other hand, our positive findings and acceptability of contact lens filter among retinitis pigmentosa patients suggest that these patients would probably wear this lens if it was on the market and we believe that this is encouraging for a contact lens firm to develop. The second limitation is a cosmetic inconvenience, as due to its full tint, the orange color outstands from the sclero-corneal limbus. The max sight lens was originally designed for performing sports and social activities and therefore, it does not important the cosmetic feature. A possible solution to this cosmetic difficulty would be to make the filter only to reach the central area of the lens. A filter diameter between 6 and 8mm would probably be enough to cover the patient's pupil without compromising the cosmetics.
The filter contact lenses seem to be a good option to improve the quality of visual of vision of patients suffering from retinitis pigmentosa. We have carried out a study with the only contact lenses filter available (although not in the market any more) but It would be of great interest to carry out a larger and longer randomized blind study with these filters or even better a to-be-developed contact lens with a better matched transmission curve. This would make it a more perfect match to the CPF glasses filter and would overcome this limitation of the study, although this contact lens would first need to be developed. Contact lens filters should also be tested for different wavelength cuts on patients suffering from other retinal degenerative diseases to evaluate their possible benefit. In conclusion, despite its limitations, our pilot study could open new pathways of research in low vision rehabilitation for retinitis pigmentosa patients.
DisclosureThe authors do not have any financial interest on the materials and instruments used in this study.
We would like to thank the Asociación Retina Madrid for their help and support during this study.





