


To evaluate the ability of the preferential hyperacuity perimeter (PHP) and the Amsler grid to detect central scotomas in Stargardt's disease and age macular degeneration.
MethodsProspective, comparative, cross-section study in which 16 patients affected with AMD and Stargardt's disease were evaluated. All patients had an optometric evaluation including refraction, best corrected visual acuity, evaluation with PHP Foresee and with the Amsler grid. The sensitivity of the macular evaluation tests (The Amsler grid and PHP) for each maculopathy was calculated.
ResultsTo detect scotomas in both macular pathologies, the PHP sensitivity is 60–70 %, while the Amsler grid sensitivity is 85–100 %. As screening methods for maculopathies, the PHP sensitivity is 83 %, while the Amsler grid sensitivity is 93 %.
ConclusionsThe Amsler grid and the PHP are both useful to detect scotomas in Stargardt's disease and AMD. As a disease screening method, the Amsler grid is useful in both conditions; however, the PHP is only useful in AMD, not in Stargardt's.
Evaluar la capacidad del perímetro de hiperagudeza preferencial (PHP) y la rejilla de Amsler para detectar escotomas centrales en la enfermedad de Stargardt y DMAE.
MétodosEstudio prospectivo, comparativo y de corte transversal en el que se ha evaluado a 16 pacientes afectos de DMAE y enfermedad de Stargardt. Todos los pacientes han sido sometidos a una evaluación optométrica que incluyó refracción, agudeza visual con la mejor compensación óptica, evaluación con PHP Foresee y evaluación con la rejilla de Amsler. Se calculó la sensibilidad de los test de evaluación macular (rejilla de Amsler y PHP) para cada maculopatía.
ResultadosEl PHP presenta una sensibilidad del 60–70 % para detectar escotomas en ambas afecciones maculares y la rejilla de Amsler, del 85–100 %. Como método de cribado de maculopatía, la sensibilidad del PHP fue del 81 %, mientras que la de la rejilla de Amsler fue del 93 %.
ConclusionesTanto la rejilla de Amsler como el PHP son útiles para la detección de escotomas en enfermedad de Stargardt y en DMAE. Como método de cribado de enfermedad, la rejilla de Amsler es útil en ambas, pero no el PHP, que se muestra útil en DMAE pero no para Stargardt.
The Stargardt's disease was described for the first time in 1909 by Karl Stargardt. It is currently the most frequent macular dystrophy, and the second most frequent retinal inherited condition after retinitis pigmentosa.1 Its prevalence is estimated to be 1/10,000 people.2 The patients report a progressive bilateral vision loss which begins when they are between 6 and 20 years old, with no previous ocular alteration symptoms.3 To keep a visual acuity (VA) over 0.5 on the decimal scale in at least one eye is a 52 % at the age of 19; a 32 % at the age of 29; and a 22 % at the age of 39.4 After decreasing to this level, the VA usually falls down quickly, and keeps stable in approx. 0.1, associated with a central scotoma.3
Age-related macular degeneration (AMD) constitutes the greatest cause of legal blindness in the Western world, in people older than 65 years of age. It is estimated 15 million American people are currently affected with AMD.5 There are two main types of AMD: the atrophic AMD, which evolves slowly along the years, causing a gradual vision loss that may lead to a central scotoma; and the neovascular AMD, characterised by the growth of choroidal neovascularization, where the most common initial symptom is the crooked and wavy appearance of the straight lines, quickly advancing up to a significant vision loss.
The Amsler grid was presented in 1947 as a technique to evaluate the central visual field in patients with macular conditions.6 It consists in a grid with a central fixation spot, on which the patient must mark scotoma areas or metamorphopsia. Its simplicity allows it to be used as a self-control, warning the patient to visit his/her ophthalmologist as soon as a change in the scotoma size and depth, or in the metamorphopsia is detected. However, this test reliability is doubtful, given a possible fixation loss, and the brain adaptation to complete scotoma areas. 7–9
The preferential hyperacuity perimeter (PHP) is a technique designed to avoid the Amsler grid problems. It is a visual field test to qualitatively measure the macular distortion areas in a non-invasive way, on the basis of the hyperacuity characteristic, i.e., the visual system ability to detect alignment errors when locating an object with regards to others in the space (Figure 1).

So far, this technology has been used to assist in the AMD monitoring, to detect changes in the visual function.10,11 Some other studies have showed that the PHP is more sensitive than the Amsler grid to detect lesions due to AMD.
The PHP research group12 studied 185 patients to evaluate the PHP ability at detecting choroidal neovascularization due to macular degeneration, and its ability to differentiate it from an average AMD stage. The results showed that the PHP sensitivity to detect new cases is a 82 %, and the test specificity to differentiate new choroidal neovascularization diagnoses in average AMD is a 88 %.
In another parallel study carried out by this group,11 they evaluated 150 patients classified in 5 groups according to their AMD type and stage. The results showed that the PHP was more sensitive than the Amsler grid to detect lesions due to AMD, in spite of a high false-positive ratio for healthy subjects.
Later on, Isaac13 evaluated 65 eyes from 65 patients grouped according to their AMD severity in another study. He found out that the device had a sensitivity of 90 %, and a specificity of 81.8 % to detect choroidal neovascularization, compared with the 70 % sensitivity and 85.5 % specificity got with the Amsler grid.
In spite of the good results achieved with this technique to handle patients with AMD, there are no studies so far to demonstrate the PHP efficacy and efficiency (Foresee PHP, Reichert, Inc. USA. 2009) for other macular retinal conditions like Stargardt's disease.
Therefore, the goal of the current study is to consider the usefulness of the PHP and the Amsler grid to evaluate the macular function in patients with Stargardt's disease and AMD.
MethodsProspective, transversal comparative study on 16 patients diagnosed with Stargardt's disease or AMD. They all had central scotomas smaller than 14°. After signing the informed consent, the patients had an optometric evaluation under photopic lightening conditions: refraction, visual acuity, PHP, and the Amsler grid.
The best-corrected, far visual acuity was evaluated using a Bailey-Lovie test. The presence of scotomas was one-eyed evaluated with the best optical compensation, using the Amsler grid with white lines on black background in one-eyed vision, and using the PHP. Before starting the test with the PHP, the patients had to go through a tutorial to avoid the possible effect of test-learning.
The sensitivity and specificity of the Amsler grid and the PHP were calculated, and compared for each condition. Likewise, there was a control group, with no disease, to check the technique reliability in their application.
Although the sensitivity and specificity are usually calculated on a validated gold standard, there is no-one to detect scotoma using VA charts, unless using methods like macular perimetry or scanning laser microperimetry. As these methods were not available for this study, our protocol defined the presence of scotoma when both conditions were present: 1) VA ≥ 0.4 logMAR, and 2) Macular condition associated to presence of central scotoma (AMD or Stargardt diagnosis). To achieve the goal of this study, it was essential to choose an objective case of scotoma definition which would allow to stimate the rate of scotoma detection with each method; thus, it was defined that the patient had scotoma when both conditions were present.
It was defined the sensitivity and specificity of the methods as scotoma detection and screening technique. To work out the sensitivity and specificity of both techniques as a screening method, it was considered a “case” when the technique was able to detect the condition in either eye.
Standard descriptive statistical techniques were used. Descriptions of mean values, proportions, sensitivity and specificity following common formules are exposed. Comparisons of proportions were performed by Chi-square test using Yates’ correction for 2-by-2 tables. All comparisons were two-tailed and performed assuming an alpha-error of 0.05 and a power of 0.8.
ResultsTwenty-six patients were evaluated, 9 affected with Stargardt's disease, 7 affected with AMD (4 affected with neovascular and for 3 with non-vascular disease), and 10 healthy controls. The patients in the Stargardt's group were 41±16 years old; in the AMD group they were 78±11 years old, and the people in the healthy control group were 57±11 years old. The VA of those patients with a maculopathy was alike in both conditions: AMD vs Stargardt's disease. The VA average in all patients was 0.6±0.55 logMAR. The average time to do the PHP was 4.23 minutes per eye.
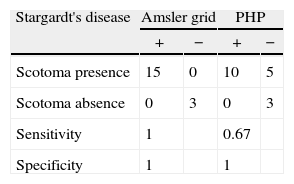
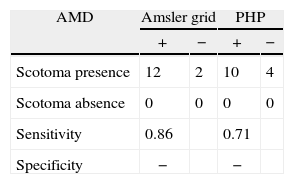
The sensitivity estimates for both techniques to detect scotomas in the central vision showed the following results: In patients with Stargardt's disease, the Amsler grid succeeded in a 100 % of cases, while the PHP detected a 66 % (Table 1) The differences in scotoma detection were statistically significant (p-value<0.05). In AMD, the sensitivity of both techniques was alike (p-value>0.05) (Table 2).
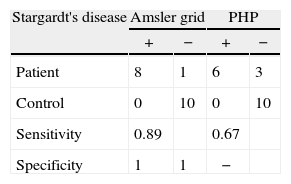
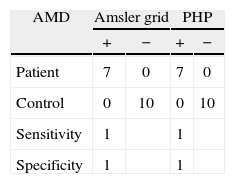
As a screening method, the Amsler grid detected a 93 % of those patients with a maculopathy; the detection percentage was alike for patients affected with AMD and Stargardt's disease (p-value>0.05) (Table 3). The PHP detected a 81 % of patients with a maculopathy, but the detection percentage was different for each pathology: a 100 % of patients with AMD, and a 67 % of patients with Stargardt's disease (p-value>0.05) (Table 4).
Out of all tests done with the PHP, a 71 % were reliable. However, it is important to point out that, while the test reliability was a 100 % in absence of disease, that percentage is considerably less when there is a disease: only a 35 % of the tests were reliable in the AMD group, and a 66 % in the Stargardt's (Figure 2).

So, we did the statistical analyses exclusively considering the reliable tests. However, the results showed no significant differences between the analyses including all the cases irrespective its reliability and the exclusive use of reliable cases.
DiscussionThe main finding of this study was the determination of the PHP sensitivity to detect central scotomas in Stargardt's disease, in comparison with the Amsler grid. This technique allows detect a 67 % of scotomas, while the Amsler grid detects a 86 % of cases. Likewise, the Amsler grid shows to be a better screening technique than the PHP for Stargardt's disease, with a sensitivity of 100 % and a 67 % respectively. Differently from the watching in Stargardt's disease, previous studies have considered the usefulness of the PHP in AMD, showing a high sensitivity in comparison with the Amsler grid, 10–13 corroborated by our own results. In this study, we found a PHP sensitivity equals to 70 % for patients affected with AMD. This result is similar to those previously published reporting a sensitivity next to 80 %.12
We are aware of the histopathological differences between both studied conditions (AMD and Stargardt's disease) and the differences in visual perception. In AMD, due to the waste products accumulated and the possible neovascularization, the affected patients will perceive a distortion in the straight lines, or metamorphopsia. However, in Stargardt's disease, due to the absence of photoreceptors in some retinal areas, there will be a lack of vision with no distortions. Nevertheless, the PHP could likely detect not only distortions (AMD), but also scotomas due to the absence of light stimulus vision (characteristic in Stargardt's). That is the reason why we decided to compare it with the Amsler grid for this type of condition, given the good results watched in AMD with this technique for the detection of both, distortion and scotomas (Figure 1).
The sole technician who performed both PHP and Amsler grid test was aware of the diagnosis. This is actually a methodological strength of the study. On the other hand, the unblinding could be considered as a disadvantage; but the possibility of biased data in these tests is so low. Moreover, it was necessary to know the patient's condition as one of the criteria to define the presence of scotoma by protocol.
We are aware of the handicap involved in the small sample size of this study, which could be considered as a first pilot one. However, there is a series of relevant findings to be confirmed in future studies with a larger sample size.
It must be considered that some of those studies comparing the sensitivity of the Amsler grid and the PHP, which show a higher sensitivity for the PHP10,11 were done using black grids on a white background. Some studies6 have shown that the original grid (black lines on a white background) offers a higher sensitivity than the modified one (white lines on a black background). In this study, to avoid over estimates in the PHP efficiency, we followed Isaac's indications13 using a grid with a black background, comparable with the used colors in the test by PHP where white stimuli are used on a black background.
Regarding the Amsler grid, we must point out that we insisted particularly in the need to do the test carefully, emphasizing its understanding and explanation of the subjective grid perception. Hence the Amsler grid sensitivity results may have been higher than in previous studies.8
The main handicap in the evaluation with PHP is the high percentage of void or unreliable test results in patients affected. This percentage is more than 60 % in AMD and more than 30 % in Stargardt's disease. This problem can be related to other field tests which must be repeated several times until a reliable result is achieved. However, this does not modify the test sensitivity results.
On the other hand, and due to the condition etiology, the AMD patients are older in average than those affected with Stargardt's disease. This difference can affect the understanding of the PHP test and the ability to do it. As a consequence, there is a low percentage of reliable tests in AMD patients in comparison with Stargardt's.
Another PHP disadvantage in comparison with the Amsler grid is the test time, estimated in an average of more than 4 minutes per eye. This means the Amsler grid is a fast, portable, cheap, accessible method, with a reasonable sensitivity and specificity at handling maculopathies.
Despite these problems, the PHP allows a qualitative and quantitative monitoring of the scotoma changes in placing and depth, in a more precise way than using the Amsler grid in AMD patients. On the other side, the PHP does not seem to be more efficient than the Amsler grid to detect the condition and scotomas in Stargardt's disease. This means it is probably a test less appropriate for diseases with photoreceptor loss, and more appropriate for diseases involving retinal degeneration.
Conflict of interestsAuthors declare that they don’t have any conflict of interests.
This study and data accumulation has been carried out in conformity with all National laws. An informed consent was obtained and the study is in adherence to the tenets of the Declaration of Helsinki.





