



Measurement of the amplitude of accommodation is established as a procedure in a routine optometric eye examination. However, clinical methods of measurement of this basic optical function have several sources of error. They are numerous and diverse, and include depth of focus, reaction time, instrument design, specification of the measurement end-point, specification of the reference point of measurement, measurement conditions, consideration of refractive error, and psychological factors. Several of these sources of inaccuracy are composed of multiple sub-sources, and many of the sub-sources influence the common methods of measurement of amplitude of accommodation. Consideration of these sources of measurement error casts doubt on the reliability of the results of measurement, on the validity of established normative values that have been produced using these methods, and on the value of reports of the results of surgery designed to restore accommodation. Clinicians can reduce the effects of some of the sources of error by modifying techniques of measurement with existing methods, but a new method may further improve accuracy.
La medición de la amplitud de acomodación se ha establecido como un procedimiento del examen optométrico ocular rutinario. Sin embargo, los métodos clínicos de medición de esta función óptica básica tienen diversas fuentes de error. Estas son numerosas y diversas, e incluyen profundidad de foco, tiempo de reacción, diseño del instrumento, especificación del punto final de la medición, especificación del punto de referencia de la medición, condiciones de la medición, consideración del error refractivo, y factores psicológicos. Algunas de estas fuentes de imprecisión se componen de múltiples sub-fuentes, muchas de las cuales influyen en los métodos comunes de medición de la amplitud de acomodación. La consideración de estas fuentes de error en la medición plantea dudas sobre la fiabilidad de los resultados de dicha medición, la validez de los valores normativos establecidos que se han producido utilizando estos métodos, y el valor de los informes sobre resultados de la cirugía diseñada para restablecer la acomodación. Los clínicos pueden reducir los efectos de algunas de las fuentes de error, modificando las técnicas de medición con ayuda de los métodos existentes, aunque el desarrollo de un nuevo método podría mejorar la precisión.
Amplitude of accommodation (AoA) is an eye's maximum range of focussing power at a particular time. It is expressed in dioptres.
In the United Kingdom (UK), AoA is the parameter of accommodation that is most commonly assessed clinically. Competence in the measurement of AoA, and in no other aspect of accommodation, is statutorily required of every aspiring UK optometrist1 and measurement of AoA is a recommended component of a routine eye examination when “clinically appropriate”.2
“Accommodation rule” is included in the list of twenty principal items of clinical equipment required for routine eye examinations in the UK.3 In North America measurement of AoA is one of the items in the Skeffington 21-point routine.4 AoA is included in the syllabi of the World Council of Optometry5 and European Council of Optometry and Optics.6
A review of the clinical measurement of AoA briefly mentioned sources of error.7 The present review describes these sources of error in more detail, facilitating better understanding of the accuracy of current methods.
The RAF Rule is the only device marketed in the UK for the clinical measurement of AoA. It was first described in 1956.8 Shown in Fig. 1, it is a graduated rail just over 0.5m in length with a handle at one end, a bifurcation at the other end to be held against the patient's cheekbones, and bearing a visual test-object. The test-object displays high-contrast black-on-white print in a range of sizes and can be slid along the rail.
Methods of measurement
Four methods of measuring AoA are encountered in clinical practice and described in the literature. They are push-up, push-down, minus lens, and retinoscopy, and are described below.
Push-upMany authors assert that push-up is the most prevalent method.9–11 In the push-up method the examiner instructs the patient to report when a test-object becomes blurred as it is brought gradually nearer to the eye. Devices which are a ruler with a sliding test-object are often used for this measurement. The RAF rule is an example of such a device. It is used as follows. When the first slight but sustained blur of the visual test-object is reported the examiner notes the position of the print on a scale marked on the rail. This scale shows the distance of the print from the eye and also the AoA as the reciprocal, in metres, of that distance. Textbooks of basic optometry generally provide fuller descriptions12–15 of the use of the RAF Rule, differing moderately from each other in some details of technique.
Push-downThe push-down method can also use the RAF Rule and similar devices. The object is moved away from the patient, from being too near for the patient to resolve, until it can be seen.
This method particularly lacks standardisation of nomenclature and of technique. For example, different authors specify differing end-points. In the earliest description16 of the push-down method the test object is moved away from the eye until the patient reports when it first becomes “quite clear” but in subsequent reports differing end-point criteria were used such as “sharp and clear”17 “just becomes clear”18 “absolutely clear”14 and “just recognisable”.15
Naming the method, and its endpoint criterion, presents some confusion. When the “just recognisable” criterion was first described19 the push-down approach was described as the “modified push-up method” which has been used20,21 in research where it has been termed the “modified push-down method”22 which resembled the “modified pull-away method” in another report.15 However, the “modified push-down method” in one report17 differed significantly to the “modified push-down method” in another22 and to the “modified push-up method” in another23 all of which used auxiliary fixed-power diverging trial lenses to extend the range of measurement.
Minus lensIn the minus lens method24,25 negative spherical lens power is added to the distance refractive correction until the patient cannot maintain the initial acuity at a pre-set viewing distance well beyond the expected near point. The AoA is given by the maximum power added while the patient can maintain focus, corrected for the viewing distance's vergence.
This method should only be used for monocular measurement and only under monocular conditions. These limitations arise because accommodation and convergence work together although the link between their operation is not rigid.26,27 Therefore, the minus lens method may induce more convergence than would be required for the viewing distance, causing one eye to over-converge, resulting in diplopia; or, if binocular viewing is maintained, the pre-setting of convergence may limit accommodation. However, unlike the push-up method and some variants of the push-down method, it only requires the resolution of an object, and so may be easier to perform, for the examiner and for the patient, than reporting on the clarity of the target.
RetinoscopyAoA can also be measured using a retinoscope. Although retinoscopy relies on the clinician's interpretation of the retinoscopy reflex, it requires no judgement by the patient. It can be used for measurement of AoA by stimulating accommodation maximally while the practitioner determines the end-point. Several investigators28–31 have described the technique in detail.
This method requires practitioner skill, judgement and experience.28,30,32 That may explain why its use has been reported less often than other methods. The need to minimise glare from the retinoscope beam in AoA measurement28,30 is another difficulty with this method.
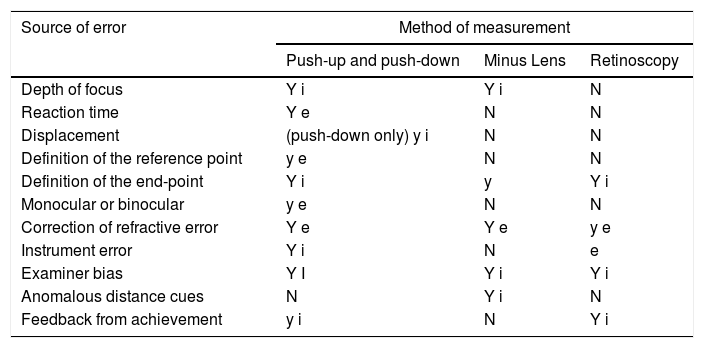
Sources of measurement errorThere are several distinct sources of error that affect current clinical methods of measuring AoA. They are listed in Table 1 which also shows the methods affected by each source of error, and are described in more detail later in this paper. Their overall effect would reduce the reliability of measurement.
Sources of error affecting the clinical measurement of AoA.
| Source of error | Method of measurement | ||
|---|---|---|---|
| Push-up and push-down | Minus Lens | Retinoscopy | |
| Depth of focus | Y i | Y i | N |
| Reaction time | Y e | N | N |
| Displacement | (push-down only) y i | N | N |
| Definition of the reference point | y e | N | N |
| Definition of the end-point | Y i | y | Y i |
| Monocular or binocular | y e | N | N |
| Correction of refractive error | Y e | Y e | y e |
| Instrument error | Y i | N | e |
| Examiner bias | Y I | Y i | Y i |
| Anomalous distance cues | N | Y i | N |
| Feedback from achievement | y i | N | Y i |
Y major effect y minor effect N negligible effect i inherent effect e effect can be eradicated.
This source of error was defined33 as the range of an object's vergence at the eye without any blur being detected. It is the result of a wide range of factors, some of which, such as diffraction, cannot be eliminated, and some, such as pupil diameter, that vary. Therefore, the contribution of depth of focus to measurement of AoA by any method that requires the recognition of blur cannot be accurately estimated. However, a review34 found that it would be likely to exceed any other source of error.
During measurement of AoA, by most methods that require the recognition of blur, the size of the retinal image of the visual target continually changes. The size is inversely proportional to the visual working-distance, and decreases slightly during measurement by the minus lens method. This size-change affects the accuracy of the measurement of AoA, since the eye's depth of focus varies with retinal image size.47
It has been proposed that depth of focus, unlike the other sources of error listed in Table 1, is both an inherent and a beneficial component of accommodation, rather than a source of error. An exploration into the depth of focus of the accommodated eye35 concluded that “the main purpose of accommodation is not to maximise retinal image quality but to form one that is good enough.” It should nonetheless be excluded when measuring AoA as depth of focus and accommodation are separate functions.
Reaction timeReaction time is a source of error that influences methods in which measurement is made while the vergence of the test object changes. This error can be limited by reducing the rate of change, although slower rates of change make the end-point less obvious so it may be harder to discern.
Reaction time is the sum of four separate components that occur in the following order when test object vergence changes past the point where noticeable blur (or, in the push-down method, either clarity or legibility) first occurs. These components are:
- 1.
the time taken to decide that the visual object appears blurred or clear
- 2.
then, the time taken to vocalise that decision
- 3.
following that, the time taken to register that message
- 4.
and finally, the time taken to stop the movement of the visual object.
Components 1 and 2 listed above depend on the patient. Components 3 and 4 listed above depend on the examiner.
Component 1, unlike the other three, is influenced by the measurement technique. It increases linearly with the rate of change of test-object vergence when measuring accommodation with the minus-lens method, and non-linearly with the rate of change of test-object distance when measurement is on a scale of distance11 because dioptric demand is inversely proportional to viewing distance. At typical maximum accommodation levels, moving the test-object one centimetre represents less than 0.1 D for a forty-year-old but about 1 D for a ten-year-old.
To reduce this error caused by the target being near to the eye at the end-point, extra minus lens power can be added in the trial frame when measuring high levels of AoA.13,15,17 Although it can be expected to reduce the reaction time error, albeit unsystematically, it would introduce error due to anomalous distance cues (another source of error, described below). Furthermore, when viewing through extra minus spectacle lenses, AoA may be influenced by refractive error.36
Therefore, it would be preferable to move the test object at a constant and slow rate of dioptres, rather than centimetres, per second. Constant rate of dioptric change (0.5D/s) for push-up measurement of AoA has been reported.37 This strategy would spread reaction-time error evenly over the range of result values but may be difficult to reliably achieve without automation. Researchers have adopted quite varied rates including 0.4cm/s,9 1cm/s,38 2cm/s,39 4cm/s with participants controlling push-down movement17 and 5cm/s20,40,41 which is so fast that the effect of reaction time on the test result could exceed one-third of the highest reported values. For example, if the near point were at 7.5cm (13.3D) movement could stop at 5cm (20D). This may be one reason why researchers from the earliest42 to present times38,39,43 obtained particularly high values, exceeding 20D, with the push-up method.
The second component of reaction-time listed above may increase if the patient feels apprehensive about the procedure and hence reluctant to declare that the test object is blurred. It may also increase if the patient is accustomed to blur.44
It would appear likely that components 2 and 3 listed above, of reaction-time, could be eliminated if the patient, instead of the examiner, were to move the target. This possibility was addressed in one study45 and not supported, as the study found slightly higher results when the participant held the target, more so when using push-up than when using push-down. However, the data were not presented to enable an estimate of the statistical significance of this result. Furthermore, an advantage of the examiner, not the patient, moving the target would be to retain some standardisation of the speed of movement.
Some early investigators41,45,46 found lower results for AoA with the push-down method than with the push-up method. Later researchers17,18 found similar results with the two methods and speculated that the earlier findings were due to the difference in reaction time between the push-up and push-down methods. Another study40 found similar results with the two methods, for 25 participants aged 10–40 years, citing other studies that found the same effect, but their push-down method used the end-point criterion of just recognising the test-object, giving large error due to depth of focus as shown by earlier research.47 The error due to depth of focus in push-down to recognition would have tended to counterbalance the error due to reaction time in push-up.
Some research11,48,49 adopted the strategy of moving the push-up test object in step changes. This would have eliminated reaction-time error because the target was stationary during measurement. However, the increased testing time of this strategy may have reduced its utility and its accuracy.
DisplacementThis error is caused by displacement of the moving visual object beyond the end-point, as follows. The end-point is registered when, in the push-down method, the observer detects that the test object's sharpness stops changing. This judgement requires comparison of sharpness at points after passing the near point, whereas in push-up the observer seeks for the sharpness to start changing, by comparing the sharpness at points before and after passing the end-point. Therefore, the end-point is displaced further from the near point in push-down because the test-object must travel further from the end-point to establish that there is no further improvement in clarity.
Displacement affects only the push-down method using the end-point criterion of clarity, causing underestimation of AoA. The displacement error would be expected to occur in the minus lens method if the end point was a change from blur to clarity, although not in the more usual procedure when the patient is asked to detect a drop in acuity13 Displacement would increase with a larger reaction time of the patient. Displacement does not appear to have been addressed in the literature.
Measurement conditionsResults with any method of measurement can be affected by the conditions of measurement. Therefore, these conditions should be specified, and standardised if possible. In measuring AoA, there are several aspects of the measurement conditions that can influence the outcome and these are discussed below using examples from AoA studies. There has been no standardisation of these or other test conditions.
Definition of the reference pointA straight line is the shortest distance between two points, and the points must be specified when giving the length of the line. When measuring AoA, a length measured from the patient is the prevalent measurement but the reference point, where the line meets the patient, has not been standardised.
Some research50,51 did not give any reference point. Others reported measuring from the target to different points such as 7mm behind the anterior corneal pole,42 13 or 14mm in front of the eye,52 the eye,53–55 the spectacle plane,16,17,25 the trial frame,28 “the corneal plane”,11 the anterior pole of the cornea,56,57 the forehead39 and the chin.58 None of these reports gave a reason for their choice of reference point. These positions, some of which (such as “the eye”) are imprecise, cover a large enough range to influence the result significantly at moderate levels of AoA and substantially more at higher levels.
Definition of the end-pointDefinition of the end-point is inherently imprecise in the retinoscopy, push-up and push-down methods of measuring AoA.
The distance of the retinoscope sighthole from the patient's eye, typically the distance to the spectacle plane, is known as the Retinoscopy Working Distance (RWD). Measurement of accommodation by retinoscopy has generally involved a shorter (often much shorter) RWD than is usual for determination of distance refractive error by retinoscopy. In reports of measurement of AoA by retinoscopy13,17,28–31,51,58–60 the RWD is the outcome measure. This would lead to imprecision, for reasons including the following:
- -
the participant is likely to move, altering the distance from participant to retinoscope.
- -
the examiner is likely to move, independently of the participant.
- -
the examiner is positioned near to the participant, perhaps as near as 10cm or less, therefore any error, such as due to movement or parallax, would be a large proportion of the measurement. In one study28 negative lenses were added to the patient's spectacle plane to increase the RWD, perhaps to reduce that error but the results did not show more precision than those of other investigations using retinoscopy.
- -
the accuracy of retinoscopy decreases unpredictably when measuring away from the visual axis32 and this error increases with nearness of a fixed-size target displacing the retinoscope beam.
- -
the measurement is taken some time after reaching the end-point.
- -
the measurement may include errors due to parallax since the ruler may have to be held away from points to which it measured. This was well illustrated photographically in the research reports that showed this detail.51,58
- -
the precision of retinoscopy is proportional to the RWD.61,62
- -
the measurement end-point may involve the subjective judgement of retinoscopic reflexes that are particularly unusual due to changes in ocular aberration with accommodation described in other research.63 This could be a reason why research51 found substantial inter-examiner variation, over 20%, in measuring AoA by retinoscopy. However, excellent reproducibility was found for this technique in a later and larger study17 in which ten examiners measured fourteen participants’ AoA using additional trial lenses to keep the RWD between 14 and 67cm. They found that 95% of the measurements were within 7% of each other.
Methods of measuring AoA that require the participant to state when a target is clear or blurred have also lacked a precise end-point. Some authors18,28,54,64,65 have reported on young participants with whom that subjective end-point would be even less reliable, including one65 who reported measuring AoA subjectively in children under two years of age.
In the minus-lens method, the end-point depends on how fine the focus must be to discern the target. Different researchers using the minus-lens method have used different target sizes, corresponding, for example, to:
Some of these would be likely to introduce imprecision of more than 1 D due to depth of focus alone, given the large reduction (and the consequent increase in depth of focus) shown26 in pupil diameter at high accommodation levels.
There is always some error in pinpointing the end-point with any measurement technique. The size of the error when measuring length is largely independent of the length being measured, such as in measuring AoA by measuring a distance. Therefore, end-point error is a higher proportion of the measurement when higher levels of AoA (i.e. shorter distances) are measured.
Fortunately, in clinical measurement of AoA, accuracy at lower levels of AoA tends to be more important than accuracy at higher levels. It can be argued that an AoA of about 4 D (more for hypermetropes reluctant to wear distance refractive correction) would cover almost everyone's practical needs.
On the other hand, accuracy in higher values may be useful in identifying change that may be of pathological significance, such as interocular difference or outliers attributable to a pathological process. Research has not yet identified a level of accuracy that might achieve these goals.
Monocular or binocularWhen not addressing interocular difference, measurement of AoA would generally be binocular, since in everyday life accommodation is normally stimulated under binocular conditions. However, binocular measurement is not always possible because of restrictions due to the measurement method as shown, for example, with the minus lens method, as described previously. This raises the possibility of error.
Measurements of one eye or of both together, under monocular or binocular stimulation, may differ by unknown amounts, because:
- -
binocular visual acuity is higher than monocular67 which may affect the speed and precision of detection of blur (or its absence) particularly in methods of measurement of AoA that are affected by reaction time.
- -
convergence induces accommodation and vice versa. Binocularity requires a fixed degree of convergence for the object distance. Therefore, the amount of accommodation may be influenced by whether the viewing is monocular or binocular.
- -
changes in pupil size, due to convergence, influence depth of focus.52
- -
more natural binocular viewing conditions may allow optimal expression of accommodation, as found in one study.68 This may be because monocular viewing can give anomalous distance cues which may cause the participant to feel somewhat disconnected from the task, and would prevent any stereoscopic sense of nearness of the target. This sense of nearness influences accommodation.83–85 One study52 found that binocular viewing gave higher results than monocular viewing. However, that investigation took place a century ago and the result was not supported by any work published since then. Moreover, another investigation45 did not show higher results when AoA was measured binocularly than when it was measured monocularly.
- -
if the AoA of one eye differs from its fellow, binocular measurement is most likely to give the higher of the two eyes’ amplitudes.
Researchers’ approach to binocularity has varied. Some54,69 stimulated and measured binocularly, or took both monocular and binocular measurements16 or did not state whether the measurements were made monocularly or binocularly.70 Those who used the minus-lens method24,51 (which, as explained above, cannot give binocular results) measured monocularly only. In at least one study50 one eye was covered. Others measured monocularly as they refracted by objective means12,51 perhaps as there were few reports of an objective method that gave results for both eyes simultaneously.
Correction of refractive errorCorrection of refractive error before measuring AoA is important because the mean spherical refractive correction must be added to the measurement (and referenced to the same point as it). Furthermore, latent hypermetropia could cause substantial and varying errors, Moreover, if spectacles are worn, the accommodative stimulus is influenced by the type and power of the prescription.71
The type of refractive error may also influence AoA but investigations have not shown the influence to be large or predictable. A study72 set out to report the extent to which AoA and refractive error were correlated. This study's 80 participants were aged 18–22 years and a mean of push-up and push-down measurements was taken. The results indicated that the sign and amount of refractive error and the manner of onset of myopia influenced AoA. The association was weak but supported by measurements of pupil diameter since hyperopic participants tended to have smaller pupils, and hence greater depth of focus, yet lower AoA. A similar effect of refractive error on AoA was found48 with the push-up method modified to reduce errors as in previous work described above11 for a similar participant group. These results suggest that refractive error is a variable that should be controlled in AoA research. However, normative studies of AoA have generally not recorded participants’ refractive error.
The approach to correcting refractive error has varied between studies and sometimes within individual studies of AoA. In one study, cycloplegic eyedrops were used52 to attempt to eliminate accommodation for the measurement of refractive error, including latent hypermetropia, except for some participants over age 46 years, whereas in another study16 cycloplegic eyedrops were instilled only for some participants younger than 20. Neither study explained why they administered a drug or gave any basis for its selective allocation. Its use could be supported by another study72 that implicitly related latent hypermetropia to AoA.
In the earliest studies of AoA42,53 correction of refractive error was not clearly described. It was not mentioned in some later research50,54,70 and its method of correction was more approximate than normal methods in a more recent study.73
Task luminanceMethods of measuring AoA that require the patient's perception of a visual target do not stipulate that the lighting of the visual task should be set to a particular level. However, target perception is influenced by the brightness of the target and of its background, as review has described.74 The influence of task luminance on AoA measurement results, independent of the eye's depth of focus, has been demonstrated75 and it has also been shown76,77 that task luminance influences depth of focus which, as discussed previously, also influences AoA measurement results.
Instrument errorThe RAF Rule is the prevalent instrument used for measuring AoA in the UK. Although it is a simple device, there appear to be fifteen sources of error, listed below, in its design and production.
Other accommodation rules that have been produced for clinical use are currently rarely used in the UK, to the authors’ knowledge, and may be expected to share some of the RAF Rule's sources of error. They use the same general principle of measurement by locating the near-point and measuring how far it is from the eye. Practitioners may improvise an accommodation rule by using a ruler and hand-held visual object.
Each of these fifteen sources of error in the RAF Rule has the potential to cause clinically significant error. The resulting errors can all be additive. Their overall effect could be addressed by revising the design although this has not enjoyed a clinically-guided change during its production-span of over sixty years. The fifteen sources of error are as follows:
- 1.
ambiguity about which part of the sliding component indicates the reading;
- 2.
ambiguity regarding which scale-graduation (or neither) the scale's numbers describe, because each number is equidistant between two graduations and indicates neither;
- 3.
uncertainty about the location of the scale's zero point, as RAF Rules appear to vary in the distance of any particular scale graduation from the cheek rest, as shown in Fig. 2 which depicts the first two RAF Rules sourced randomly by one of the authors;
- 4.
the slider's opaqueness, obscuring interpolation between graduations;
- 5.
the effect on the location of the scale arising from inter-individual differences in facial anatomy, at any given distance, d, of the cheek rest below the corneal vertex;
- 6.
the effect of not specifying d, mentioned in point (5) above, as facial anatomy is not perpendicular to the RAF Rule;
- 7.
the effect of not specifying d, as facial anatomy varies between people;
- 8.
the effect of not specifying the distance d on point (14) below;
- 9.
the variability of luminance contrast of the text. The contrast could be standardised by backlighting the text;
- 10.
the limits of the scale. Values of AoA higher than the measurement range of the unmodified instrument have often been reported22,37,38,42,78;
- 11.
the variable location of fixation within one line of target print, since different letters in the line, which is 27mm long, are at different distances from either eye, producing differing accommodative demand of up to 0.25 D when measuring approximately 6 D of accommodation with the RAF Rule. Higher errors occur at shorter target distances;
- 12.
the effect of target detail size, through depth of focus34;
- 13.
the effect of scale interval linearity, through reaction time as previously discussed;
- 14.
the variability of rail declination. This is shown in Fig. 3, two pictures taken of the instrument in routine clinical use, showing how the rule may be held above or below the primary position of gaze.


The declination influences the result, for the following reason. There is a quadrilateral formed by the corneal vertex or other reference point of measurement, the test object, the measurement index on the slider, and the midpoint between the cheek rests. This quadrilateral is generally irregular and its shape varies with the measurement and the Rule's position. The effect of declination can be calculated trigonometrically: at median levels of AoA the tilt of the Rule shown in the upper photograph in Fig. 3 would give a measurement of AoA approximately 1 D lower than if the Rule were tilted as in the lower photograph.
There is no consensus on how the RAF Rule should be held. Guidance varies between authorities12,13,15 sometimes picturing the instrument tilted substantially down in use.
Furthermore, there are reports that declination of gaze influences AoA.79,80 Moreover, if the rail is tilted too far down, the normal narrowing of the palpebral aperture in downgaze may reduce pupil area, increasing depth of focus. Where a phoropter is used in AoA measurement, its rail is horizontal.
- 15.
The other source of error inherent in the design of this instrument applies to monocular measurements. The error is that the rule is placed on the midline between the two eyes, rather than on the visual axis of the eye being measured.45 This would inflate results by an amount that can be trigonometrically estimated as about 5% at the highest levels of AoA and approximately proportionately less at lower levels, so it is not as large as some other errors listed above. Correction for this source of error has been precise,45,72 approximate16 or missing42,78 with the latter studies reporting higher upper measurements of AoA than other studies.
In the above list of sources of error arising from apparent weaknesses in the design and production of the RAF Rule, published information was not found for items 1–13.
Measurement with the minus-lens method minifies the target because it is viewed through negatively-powered lenses. The negative power, and hence the minification, is greater at higher levels of measurement. The minification has been cited14,41 as a possible source of error. No theoretical or empirical reports were found of the size of this error being clinically significant.
When viewing through spectacle lenses, AoA may be influenced by refractive error, the degree of influence depending on the power of the lens.36 This may be an additional source of error with the minus-lens method.66
Examiner biasThis is a source of error in any measurement that is not fully automatic. The practitioner examining the patient will often, and perhaps always, have an expectation of approximately where the measurement end-point should be. That expectation, and inevitable differences in technique between practitioners, may influence how the measurement is taken (e.g., the visual object's speed), which may in turn influence the result. It may affect naive patients more.
Research of accommodative response81 and fixation disparity82 has shown that the exact wording of instructions can influence the results of measurement. Significant differences between five different examiners’ results for push-up measurement of AoA were found and attributed to possible differences between examiners’ measurement techniques.38
Examiner bias may be suspected particularly when the general level of methodological rigour appears low and the results are not corroborated elsewhere. A normative study in South Africa specified no method of measurement and discussed the conclusion that AoA was influenced by race70 and another found a 5 D difference between amplitudes of accommodation of urban and rural children aged five to eight, using a method described only briefly and in unspecific terms.54
Anomalous distance cuesAwareness of a visual object's distance influences accommodation.83–85 In comparing methods of measuring AoA, the test object is further away in the minus lens method and measurement conditions are monocular, reducing awareness of proximity. Other methods give higher results, to differing extents.28,41,46,59 The lowest values of all investigations of AoA were obtained using the minus-lens method with objective measurement (simultaneous autorefraction).56
Results for AoA with the minus-lens method were significantly higher when using a shorter viewing distance.66 Measurement was monocular so the difference was not attributable to the induction of extra accommodation by extra convergence. The authors attributed the effect to proximal accommodation.
With particularly careful methodology it was found that accommodation measured with either the push-up or the push-down methods was higher when the participant grasped and guided the target than when the target was held and guided by the examiner.45 No reason for this finding has been demonstrated but it could have been due to various psychological factors including increased awareness of proximity when the participant connected with, and controlled, the target. Accommodation rules such as the RAF Rule may therefore give higher measurements because of reasons including their physical contact with the patient.
Feedback from achievementMethods of measurement that reward patients striving to improve their performance by feeding back how well they are achieving discernment of detail, encouraging effort to achieve the best visual performance, tend to give higher results for AoA and other aspects of accommodation.86,87 Encouragement of effort is advised for even the most basic subjective assessment of visual performance.88
The reward for effort differs in different methods. Obtaining nearness, the goal for the patient using the push-up method, probably offers little motivation to produce higher results, although this may depend on the instructions given. Maximum accommodative effort would be more likely to meet the challenge of discovering detail encountered in methods such as push-down with the “just recognisable” end-point, the minus lens method, and retinoscopy with a suitable visual object such as a Snellen chart reduced to about 5% of its usual size.
ConclusionsMany sources of error have been described in existing methods of measuring AoA. It is noteworthy that so many sources of inaccuracy can be identified in a single-parameter, long-established, basic and ubiquitous clinical measurement.
The sources of error differ considerably in their nature and in the magnitude of their effect. Some are relatively systematic while others are of unpredictable size or direction or both, some affect lower readings more than higher readings and vice versa, some affect only certain methods of measurement, some affect different methods differently, some are due to human factors of the patient or of the practitioner, some are due to factors of the equipment, or of the method, used for measurement. Their overall effect greatly reduces the validity of clinical results with current methods.
The measurement errors caused by these many sources of error can all be reduced (and a few of them can be eradicated) by better attention to measurement technique and by the standardisation of equipment and methods. However, such improvements to existing methods would generally increase the complexity, duration and difficulty of the measurement.
Presbyopia is normal for older people and cures for it would find widespread application. Surgical cures for presbyopia have long been sought. Compared to optical management of presbyopia they are risky and can be costly, but on review89–91 they showed limited success. Their validation would require accurate and reliable clinical measurement of AoA. In the future, it seems likely that improvements in the measurement of the AoA may have applications in older patients as well as people conventionally described as pre-presbyopes.
Guidance for cliniciansThe individual practitioner can take certain steps to reduce AoA measurement-error in current clinical practice, relatively effectively and easily. For example, visual object detail should be close to the limit of resolution at the near point, and the method used should be recorded with the measurement.
When measuring with devices using a ruler with a sliding visual object, such as the RAF Rule:
- -
movement of the slider should be slow, perhaps approximately one dioptre per second;
- -
during measurement the patient should receive positive feedback for effort;
- -
the rule should be held in the primary position of gaze;
- -
in push-down, the end-point criterion of sharp focus should be adopted;
- -
measurement should be to a clear, precise reference point such as the corneal vertex;
- -
any correction for refractive error should be referenced to the same point;
- -
the practitioner should check the individual rule's accuracy by measuring the near-point distance with a separate rule;
- -
the practitioner should consider taking a first measurement using the push-up method and then moving the slider away from the patient to obtain a push-down measurement. The recorded AoA would be the average of these two values.14,15
When using the minus-lens method, the visual object should be as close to the eye being measured as feasible, and minus-lens power should be changed slowly. For retinoscopy, the practitioner may consider reducing error by using a normal working distance such as 67cm, adding minus lenses in the trial frame for the refracted eye. This possible method does not appear to have received research attention.
Notwithstanding these possible improvements to existing methods, a new AoA-measurement method has been sought by the current authors. It is intended to be acceptable in clinical practice and to provide more reliable measurement. The authors hope to publish a description of this new method and to report initial results obtained with it.





