

An indication of the laterality of ocular dominance (OD) informs the clinical decision making process when considering certain ophthalmic refractive and surgical interventions. Can predictive reliance be assured regardless of OD technique or is the indication of a dominant eye method-dependent?
MethodsTwo alternative OD test formats were administered to a group of 72 emmetropic healthy young adult subjects: the ‘hole-in-card’ test for sighting dominance and the ‘+1.50D blur’ test for sensory dominance. Both techniques were chosen as being likely familiar to the majority of ophthalmic clinicians; to promote and expedite application during the examination routine neither test required specialist training nor equipment.
ResultsRight eye dominance was indicated in 71% of cases by the sighting test but in only 54% of subjects using the sensory test. The laterality of OD indicated for the individual subject by each technique was in agreement on only 50% of occasions.
ConclusionsReasons are considered for the poor intra-individual agreement between OD tests, along with an item of procedural advice for the clinician.
Una indicación de la lateralidad de la dominancia ocular (DO) contribuye al proceso de toma de decisiones clínicas a la hora de contemplar ciertas operaciones quirúrgicas y refractivas oftálmicas. ¿Puede garantizarse la fiabilidad predictiva independientemente de la técnica de DO que se utilice, o la indicación de un ojo dominante depende del método?
Métodosse administraron dos formatos de prueba de DO a un grupo de 72 sujetos jóvenes, adultos, sanos y emétropes: la prueba del agujero en la tarjeta para la dominancia direccional y la prueba de “desenfoque de +1,50 D” para la dominancia sensorial. Ambas técnicas se seleccionaron porque se consideró que la mayoría de clínicos oftálmicos las conocerían por igual. Para fomentar y agilizar su aplicación en las exploraciones sistemáticas, ninguna de las pruebas requirió ningún equipo ni formación específica.
Resultadoshubo indicios de dominancia del ojo derecho en el 71% de los casos según la prueba de visión y solamente del 54% en los sujetos que se sometieron a la prueba sensorial. La lateralidad de la DO indicada para los sujetos según cada técnica coincidió solamente en el 50% de los casos.
Conclusionesse consideran los motivos de la baja coincidencia en un mismo individuo entre las pruebas de DO, junto con un artículo de recomendaciones del procedimiento para el médico.
Although the human anatomy is arranged symmetrically about a central vertical axis, the majority of persons will use one side of their body with greater frequency, facility or skill than the other. From this universal observation has emerged the functional concept of laterality dominance,1 demonstrated in physical terms as an habitual writing hand or perhaps a preferred ball-kicking foot. Notwithstanding the uniquely bilateral cortical representation of either eye, a similar distinction has arisen with respect to the ocular system: the majority of individuals will use a preferred eye for particular uni-ocular tasks or under specific viewing conditions.
Contrary to popular belief the laterality of a preferred eye is not linked or matched to limb preference, and is also not reliably indicated by habitually superior visual acuity (VA) of one or other eye.2 Furthermore, it has come to be realised that laterality of eye dominance is not as functionally rigid as the term might imply, instead varying in degree or presence depending upon test circumstances.3–5
Nevertheless, there arise clinical situations where the demonstration of a preferred eye is a necessary precursor to any proposed ophthalmic therapy or treatment. These occasions include the prescribing of symptom-relieving optical prism as a supplement in corrective spectacle lenses,6 where all (or the greater part) of the prescribed prism is located before the non-dominant eye. The knowledge of an individual's OD is useful when considering the expediency of a ‘monovision’ approach to temporary or longterm unilateral refractive correction with contact lenses or surgery.7 The monovision technique was initially devised for the convenience of presbyopic contact lens wearers,8 but ocular surgery has embraced this approach in conjunction with intra-ocular lens implantation and (laser) refractive procedures with a high rate of success and degree of patient satisfaction across the several studies now reported.9,10 In monovision the dominant eye is usually corrected for distance and its companion for near: it is considered that the sight of the dominant eye will be less easily suppressed by the relatively blurred image in the non-dominant eye.7 It is also worth remarking that the ophthalmic clinician with a preferred viewing eye might (in the early years of a career) experience difficulty when using monocular equipment (e.g., an ophthalmoscope) to examine a patient's eye or ocular adnexa or when setting up and aligning instrumentation for ophthalmic measurement (e.g., a slit lamp-mounted Goldmann applanation tonometer). It is usually the case that experience will moderate or overcome initial difficulties.
Laterality of ocular dominance might be determined in several ways.11–13 The question arises as to which approach could be considered the most appropriate. Should the test reflect visually guided behaviour using, for example, a sighting or visual alignment task? Alternatively, should reliance be placed on an assessment of the sensory modality using tests of spatial vision or perhaps an unilateral optical blurring or stereo suppression technique? And if both types of test were undertaken on an individual, would the ocular laterality results be in agreement? On this latter point consensus is lacking: while several authors have reported disagreement between the outcome of the alternative OD test approaches,14–18 others have disputed this conclusion.19,20
Given the advisabilty of establishing the existence and laterality of any eye preference before attempting an unilateral optometric or ophthalmological intervention, the results of a concise comparative investigation are reported here using two specific OD tests, one sighting-based and the other sensory.
MethodsSubjectsA group of 72 (51% males) normally sighted emmetropic binocular subjects was assembled. All individuals were aged between 16 and 40 years, in an attempt to minimise the acknowledged deterioration of binocular function with advancing age.21 All participants were in good general and ocular health, and not taking any prescription medications with known oculo-visual side effects. Subjects habitually recorded good distance acuity of <0.00logMAR (better than 6/6 Snellen) unaided in either eye: nevertheless, for the study accurately centred full-aperture trial case lenses were used to achieve optimal acuity (an important procedural consideration).22 Each subject also demonstrated good binocular function and normal stereopsis. Natural pupil sizes were retained, and all testing was undertaken in an uniformly-lit room receiving solely artificial illumination.
This prospective study satisfied the tenets of the Declaration of Helsinki: following an explanation of the short term non-invasive procedures to be undertaken each subject gave verbal consent to their participation in the study. No financial inducement or reward was offered.
Ocular dominance testsA multitude of tests have been proposed for the determination of OD.13 Many are simply variations on a theme or require the use of specific equipment. For this concise clinical study only two techniques were selected for application, each of which has, in comparison to alternative formats, a track record of intra-test predictive consistency: viz., a widely used simple sighting alignment test,11 and a monocular optical blurring test which temporarily introduces a viewing situation akin to monovision.15 Both tests have the additional advantage of being familiar to the majority of practising clinicians and require no specialist instrumentation.
Sighting OD was established by three successive consistent trials of the ‘hole-in-card’ test. With both eyes open the subject held, with both hands and comfortably at arms’ length, a rectangular piece of card with a circular hole cut at its centre: through this aperture the subject viewed a small but easily visible single letter on the 6m-distant logMAR test chart. The examiner then alternately occluded either eye of the subject, and the dominant eye was recorded as the one that continued to see the letter when its companion was covered.
Sensory OD was determined by three successive consistent trials of the ‘+1.50D (dioptre) blur’ test. The subject was instructed to look binocularly at the smallest subjectively detectable line on the externally illuminated 6m-distant high contrast logMAR letter chart. A +1.50D spherical full-aperture trial case lens was then held by the examiner before one eye of the subject for a few seconds, removed and then held before the other eye for a similarly short period. The subject had to decide which of the two situations produced an uncomfortably blurred visual percept. If the visual disruption was judged greatest with the lens before the right eye then that eye was recorded as the dominant one, and vice versa. For the sensory dominant eye thus deduced the monocular logMAR visual acuity as reduced by the +1.50D blurring lens was recorded while the fellow eye was occluded. After allowing a few seconds for readjustment without the optical blur the optimal monocular logMAR acuity for that same eye was established.
Statistical analysisAll statistical analyses were undertaken using Statistica/Mac software (v4.1: StatSoft, Inc., Tulsa, OK, USA). Non-parametric techniques, including the Chi-Squared test, were employed to evaluate the relationships between the numerical frequency distributions of the ocular lateral preference data. Parametric tests, including the t-test, were used for comparative assessment of the (normally distributed) logMAR acuity data and age distributions. On all statistical tests p<0.05 was considered significant.
ResultsThe subject group (n=72: mean age 29.0±7.4 years) comprised 51% males (n=37: mean age 28.9±7.4 years) and 49% females (n=35: mean age 29.2±7.5 years). Age distributions of the genders were not statistically significantly different (p=0.8). Mean optimal monocular VA for the sensory dominant eye across the group was −0.089±0.052logMAR (6/4.9 Snellen), with no statistically significant difference between the mean acuity of right or left dominant eyes (p=0.6) and no statistically significant gender-based acuity differences (p>0.4).
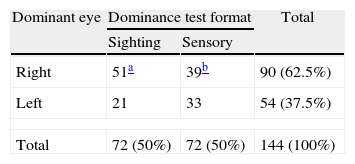
Table 1 summarises the OD outcomes recorded with the two alternative dominance test formats across the whole study group. Because distributions for male or female subjects were not statistically significantly different within and between tests (p>0.6) combined-gender numerical data are presented and analysed here.
Assessment of the raw data indicated that there was inter-test agreement of OD laterality in only 50% (36 of 72) of instances. Seventy-one percent (51 of 72) of individuals were identified as right eye dominant using the sighting test, while only 54% (39 of 72) of persons were right eye dominant with the sensory (monocular blur) test. This represents a statistically significantly different outcome (p=0.04) between tests.
As an aside, it was found that the introduction of +1.50D of spherical monocular spectacle blur under these test conditions reduced the group mean logMAR acuity for the sensory dominant eye of these young adult subjects to +0.705±0.096 (6/30.4 Snellen) from an optimal level of −0.089±0.052 (6/4.9). As an illustration (and ignoring any effect of variables such as pupil size)23 this approximately 0.8 log unit loss corresponds to a theoretical deterioration in clinical Snellen VA of 6/4 to 6/25, or 6/5 to 6/32, or 6/6 to 6/38. A pragmatic implication of this quantitative observation will be considered later.
DiscussionWe specifically investigated OD under conditions of distance (6m) fixation: we cannot speculate here whether the same outcome would have been obtained for near viewing.24 What can be stated is that the value of 71% right OD found for these subjects using the sighting test is in accord with the proportion recorded in larger population-based studies reported in the literature.1 The much lower value of 54% right eyedness obtained when applying the monocular blur test to these same individuals is striking but not unrecognised,15 as is the magnitude of the level of agreement (only 50% here) between the two alternative techniques across this subject group.
These incongruent OD test outcomes are in accord with similar but larger and more extensive comparative studies (most recently Seijas et al.15) in suggesting that alternative (e.g., sighting versus sensory) OD techniques show poor intra-subject agreement. Recent reviews of the phenomenon of OD, including its identification and a consideration of the significance of eye dominance within human visual perception, have suggested a more circumscribed role for a preferred eye than the burgeoning research literature on the topic might imply.4,25 Put succinctly, perhaps a so-called ‘dominant eye’ is simply that eye which is used by habit, preference or circumstance when viewing conditions permit only monocular or unilateral fixation. Furthermore it has been suggested on more than one occasion that perhaps a strong individual indication of OD might even prove to be a barrier to that person's subsequent successful tolerance of monovision.15,26
Under clinical circumstances, when an unilateral ophthalmic/optical treatment is to be applied, does an absolute sighting task or a relative sensory technique provide the most appropriate indication of OD? Recognising that the human visual system is habitually binocular, might tests that permit the maintenance of (a degree of) binocularity during ocular preference testing be desirable?27 However, a lack of significant sensory dominance in the normal visual system has been claimed,14 in which case indications of OD derived from sensory techniques may not prove a useful basis for ophthalmic clinical decision-making. Then again, given the evolving evidence-base that suggests OD might be considered a situation-driven preference,4,25,27 might a sighting technique better reflect the reality of OD? Finally, it has to be acknowledged that although the monocular refractive blur procedure (temporarily) produces a clinical situation akin to monovision correction the simplicity of the ‘hole-in-card’ test, possibly combined with peer-imitation based upon the published literature, probably accounts for this technique's popularity and frequent selection to indicate a preferred eye in the clinic or consulting room.
As a final point, a practical proposal arises from this present work. A recent study15 that investigated a battery of sighting and sensory OD tests reported a degree of OD uncertainty in >11.5% of cases using the optical blur test as compared to no equivocation using the ‘hole-in-card’ approach. Those authors used +1.00D of optical defocus which, in young adult subjects, has been shown to produce an approximately 0.4 log unit acuity loss28; whence 6/4 Snellen reduces to 6/10, 6/5 to 6/13, and 6/6 to 6/15. The +1.50D blur utilised in the present study produced a larger (0.8 log unit) acuity loss in our subjects (see Section “Results”), and in doing so appeared to remove subjective uncertainty as to the preferred laterality: unequivocal responses were recorded across subjects. It is thus suggested that a blurring lens of this greater refractive magnitude should preferably be used if this particular sensory OD test is applied to clinical subjects.





