

To understand the potential barriers, motivators and enablers in dispensing multifocal contact lenses (MFCL).
MethodTwo focus group discussions were conducted to design questionnaires regarding the prescribing habits for multifocal contact lenses (MFCL). Questions on potential barriers and motivators were included. The questionnaires were distributed among 133 eye care practitioners across Mumbai, India. Practitioners fitting one or less patient per month with MFCL completed the survey describing potential barriers, while those who prescribed more MFCL's per month completed the survey describing enablers and motivators.
ResultsResponses from 102 practitioners were received. Most common potential barriers in prescribing MFCL were increased chair time (75%), lack of readily available trials (69%) and limitation in power range (63%). Lack of awareness among patients (90%) was the most common barrier from patients’ outlook. Professional satisfaction (88%) and better business proposition (82%) were observed as main motivators while availability of the trials (84%) and correct patient selection (82%) were the major enablers. Graduate Optometrists felt dispensing MFCL did not offer a good business proposition (p=0.02). Experienced practitioners were observed to be least motivated (p=0.01) and believed that their patients found these lenses expensive (p=0.02).
ConclusionTo enhance the MFCL practice, barriers like lack of awareness and limitations in power range must be addressed. Trial lens availability may motivate practitioners to prescribe MFCL. Further probing is required to understand lack of motivation among experienced practitioners.
Comprender las barreras potenciales y los factores motivadores y facilitadores de la dispensación de lentes de contacto multifocales (MFCL).
MétodoSe llevaron a cabo dos debates a fin de diseñar los cuestionarios relativos a los hábitos de prescripción de las lentes de contacto multifocales (MFCL). Se incluyeron cuestiones sobre las barreras potenciales y los factores motivadores. Dichos cuestionarios fueron distribuidos entre 133 profesionales de cuidados oculares en Mumbai, India. Los profesionales que adaptaban una o menos lentillas multifocales al mes completaron la encuesta que describe las barreras potenciales, mientras que aquellos facultativos que adaptaban más lentes de contacto al mes completaron la encuesta que describe los factores facilitadores y motivadores.
ResultadosSe recibieron respuestas procedentes de 102 facultativos. Las barreras potenciales más comunes de la prescripción de MFCL fueron el incremento del tiempo de consulta (75%), la falta de disponibilidad de lentes de prueba (69%) y la limitación del rango de potencia (63%). La falta de concienciación de los pacientes (90%) fue la barrera más común desde la perspectiva del paciente. Como principales factores motivadores se observaron la satisfacción profesional (88%) y la mejor propuesta comercial (82%), mientras que la disponibilidad de lentes de prueba (84%) y la correcta selección del paciente (82%) fueron los principales factores facilitadores. Los Optometristas Graduados pensaron que la dispensación de MFCL no ofrecía una buena propuesta comercial (p=0,02). Se observó que los facultativos experimentados estaban menos motivados (p=0,01), y pensaban que sus pacientes consideraban que estas lentes eran caras (p=0,02).
ConclusiónPara mejorar la práctica de las MFCL, deben abordarse las barreras tales como la falta de concienciación y las limitaciones del rango de potencia. La disponibilidad de lentes de prueba puede motivar a los facultativos a prescribir MFCL. Hace falta investigación adicional para ayudar a comprender la falta de motivación entre los facultativos experimentados.
With the aging of the population globally, the contact lens industry perceived tremendous potential in the presbyopic market. Efforts were thus made to create better corrective lens options for these patients. The concept of bifocal contact lenses has a history since 1938, when Feinbloom from New York described a segmented Bifocal CL and a Trifocal CL (Moss, 1962). In 1957, DeCarle in London developed simultaneous-vision bifocal CLs that were free from the problem of rotation, which became the basis for current bifocal CL (DeCarle, 1989). In the latter half of the 1980s to the 1990s, nonspherical progressive MFCL (Stein, 1990) and diffraction CL (Freeman and Stone, 1987) were developed, and a large number of bifocal CLs were made. Today, a wide range of both rigid gas permeable and soft multifocal contact lenses (MFCL) – as an option for correcting presbyopia – are available globally.1
Lens design, lighting and contrast are known to affect the visual performance of these lenses. The early MFCL designs were found to decrease contrast sensitivity and stereoacuity for the patient thus affecting the adaptation to these lenses.2–4 Studies with lenses designed to overcome these issues have shown that high contrast acuity is not significantly affected with bifocal contact lenses.5 Recent study done with simultaneous MFCL lens design showed good results in achieving required visual acuity and visual performance under – real life conditions.6 Few studies also reported that advances in the lens design found no significant decrease in stereoacuity with MFCL as compared to spectacle correction.7,8
Considering these advancements and better patient satisfaction with the newer designs, MFCL are expected to be the preferred choice for correcting presbyopia as compared to other contact lens correcting options.8
However, a survey on contact lens prescribing patterns conducted in India showed that only 33% of presbyopes were prescribed MFCL, while the recent global survey showed that half of all patients in the presbyopic age range are prescribed multifocal contact lenses, while only 10% receive a monovision correction.9,10 Few studies also observed that practitioners preferred fitting monovision lenses over MFCL, which may be due to the ease of fitting and availability of wide power range.8,11,12
There is no clarity on the factors governing the prescribing and dispensing of MFCL. This study was thus conducted to get a better understanding of the barriers perceived by practitioners in India, which could be the major reason to limit the popularity of these lenses. We also wanted to identify the motivators and enablers from the practitioners who have been successfully dispensing these lenses and the impact of factors like, years of experience, type of practice and different optometry training levels contributing to the prescribing of these lenses. As optometry is not a regulated profession, these factors could also play a role in contact lens dispensing in India. Understanding and addressing these factors might help in exploring the untapped market of MFCL.
MethodologyTwo focus group discussions were conducted for designing the research questionnaires. One group consisted of 12 eye care practitioners (ECPs) who regularly dispensed MFCL (on average minimum two patients per month), while the other group consisted of 12 ECPs who did not, or occasionally, dispensed MFCL (on an average one or less than one patient per month). Barriers, motivators and enablers for dispensing MFCL were discussed and documented from both the practitioner and patient's perspective. All the discussed points covering the barriers, motivators and enablers were rated by the two groups from being the most common and relevant to the least common and relevant points responsible for the limitation in dispensing MFCL. All the highly rated points were considered and incorporated in designing the final questionnaire, which was used during the survey.
The final questionnaire was distributed among 133 practitioners across Mumbai, India, through either email with prior telephonic explanation about the survey or through personal distribution of the questionnaire with explanation prior to enrollment. Basic demographic data of the practitioners, including their qualification and the years of experience, were documented after obtaining their consent. Practitioners fitting one or fewer patients with MFCL per month completed survey A which described the potential barriers in fitting MFCL, while practitioners fitting two or more MFCL per month completed the survey B describing the motivators and the enablers for dispensing MFCL. This questionnaire included questions for ECPs from both practitioner and patient's perspective. The responses of the practitioner were rated on a five-point scale (from strongly disagree to strongly agree) based on their level of agreement to the statements in the survey. Data were manually entered in an excel sheet and was used for final analysis.
Statistical analysisThe means and standard deviation for the linear variables and proportions for categorical variables were estimated. The difference in the mean was tested using unpaired t-test and difference in the proportions was tested using the chi-square test or Fisher's exact test (for low expected cell counts). p value <0.05 was considered to be statistically significant. The data entered in MS Excel were converted to Stata for analysis using Stata Version 11.
Results102 (77%) out of 133 ECPs successfully completed the survey. An almost equal number of respondents completed each survey, 51% of ECPs completed survey A while 49% completed survey B. Two-thirds of the respondents were males (66.67%) with a mean experience of 11±8 years as compared to that seen in female respondents which was 8±5 (p=0.03). The majority of practices represented were stand-alone (81%) as compared to (19%) retail chain outlets.
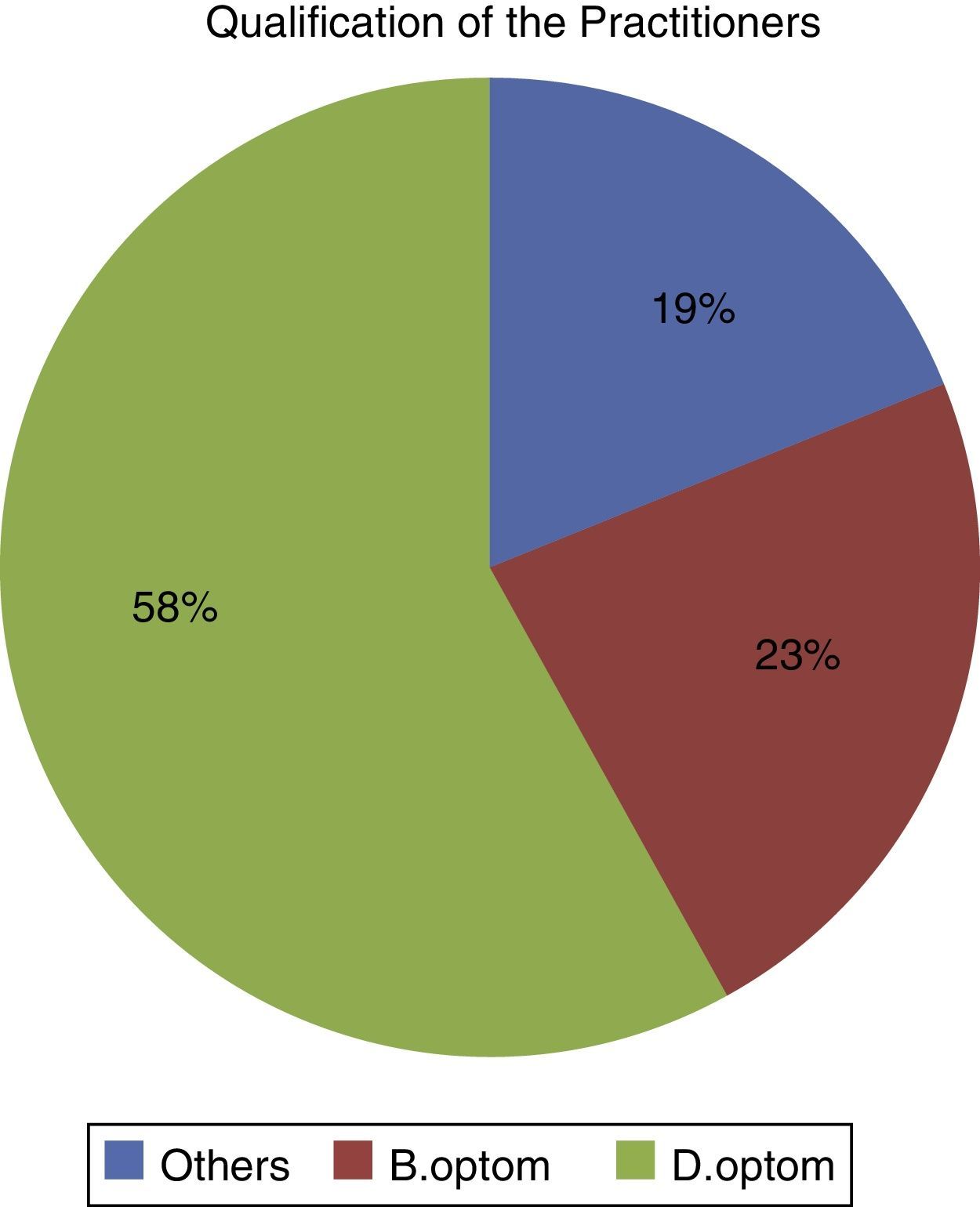
Most practitioners had undergone formal optometry training – 23% were graduates who had completed a degree program or more in optometry, while 58% completed their diploma program in optometry and 19% practitioners were observed to be non-optometry qualified practitioners (Fig. 1).

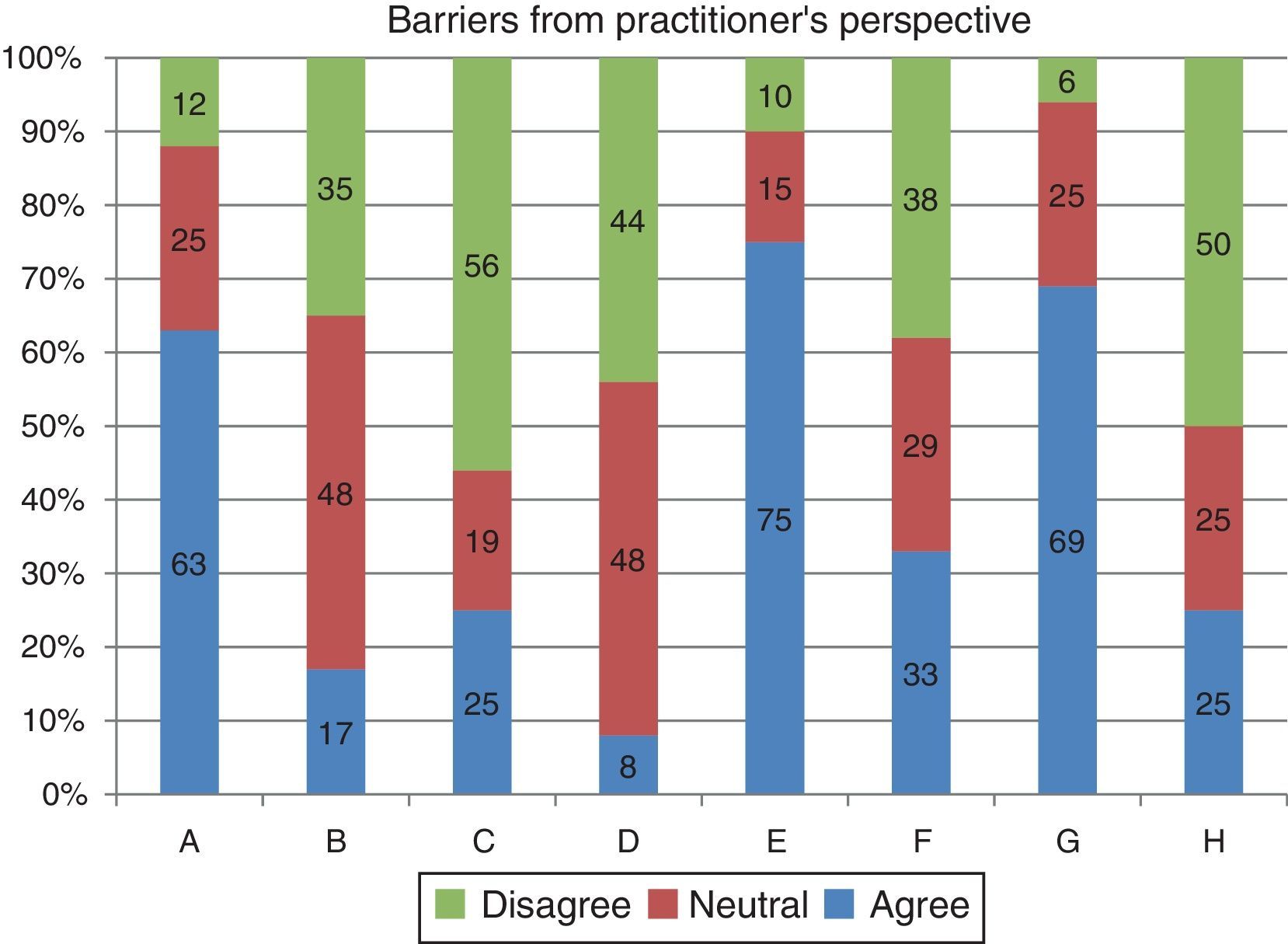
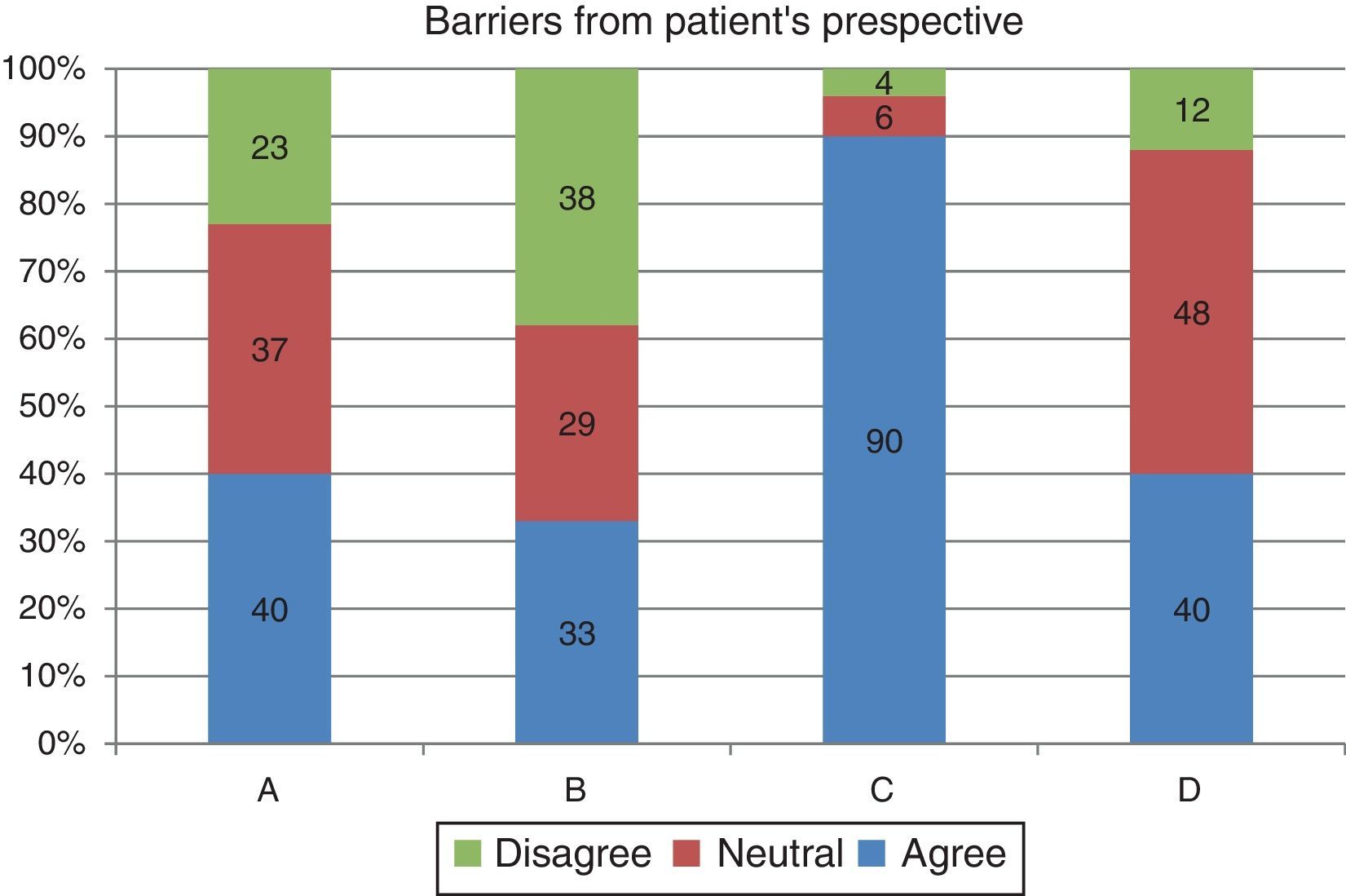
The most common barriers in prescribing MFCL from a practitioners’ perspective were increased chair time (75%), lack of readily available trial lenses (69%) and limitation in power range (63%) (Fig. 2). The majority of practitioners reported that lack of awareness (90%) was the major barrier from patient's perspective, while cost was the secondary barrier (48%) (Fig. 3).
 limitation in power range availability, (B) lack of confidence, (C) lack of knowledge and skills, (D) do not provide good business proposition, (E) increased chair time, (F) lack of motivation, (G) trial lenses not readily available and (H) lens material not suitable for long hours.")
Responses from survey A: (A) limitation in power range availability, (B) lack of confidence, (C) lack of knowledge and skills, (D) do not provide good business proposition, (E) increased chair time, (F) lack of motivation, (G) trial lenses not readily available and (H) lens material not suitable for long hours.
 lack of motivation, (B) unsatisfactory vision with multifocal contact lenses, (C) lack of awareness and (D) expensive.")
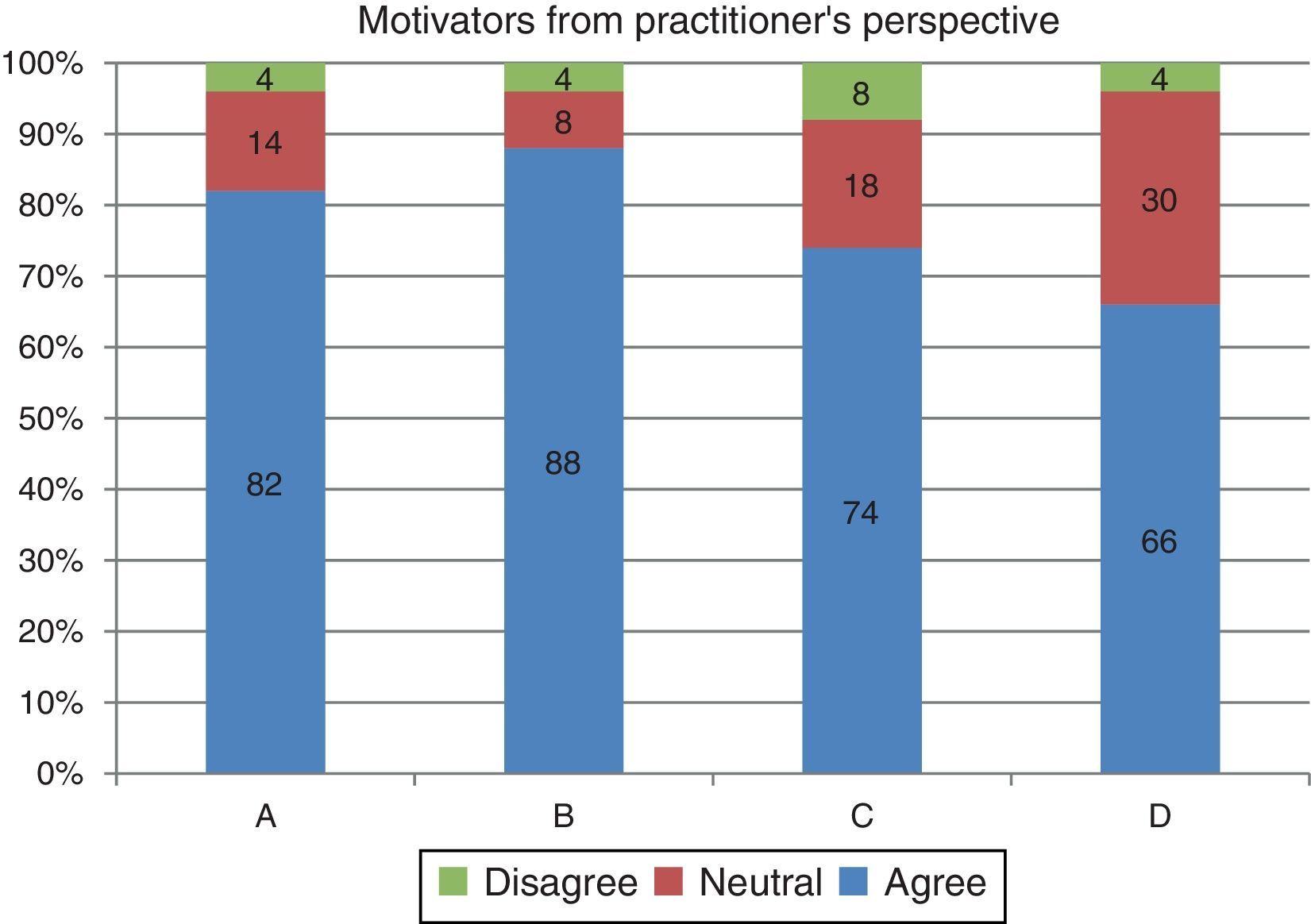
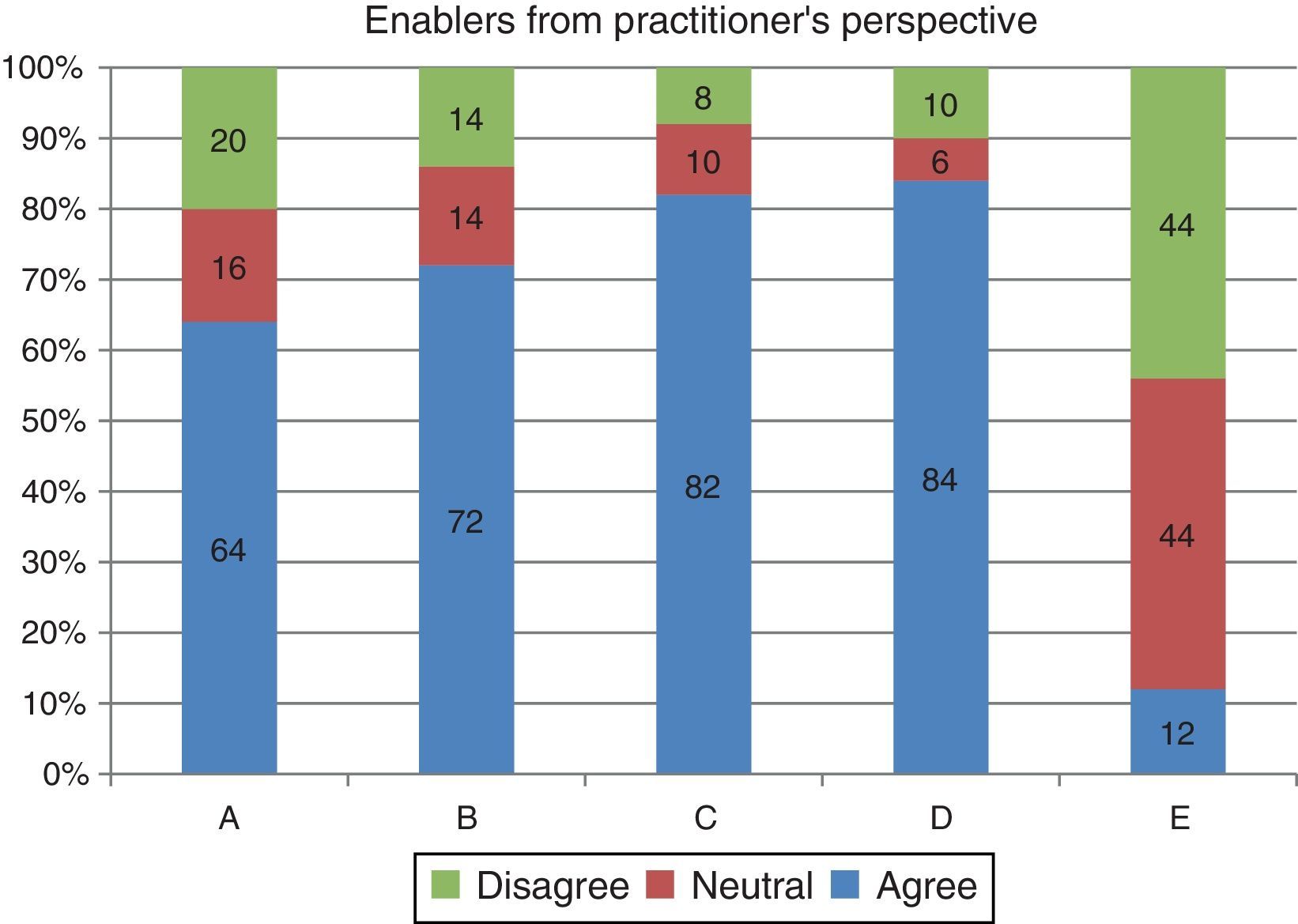
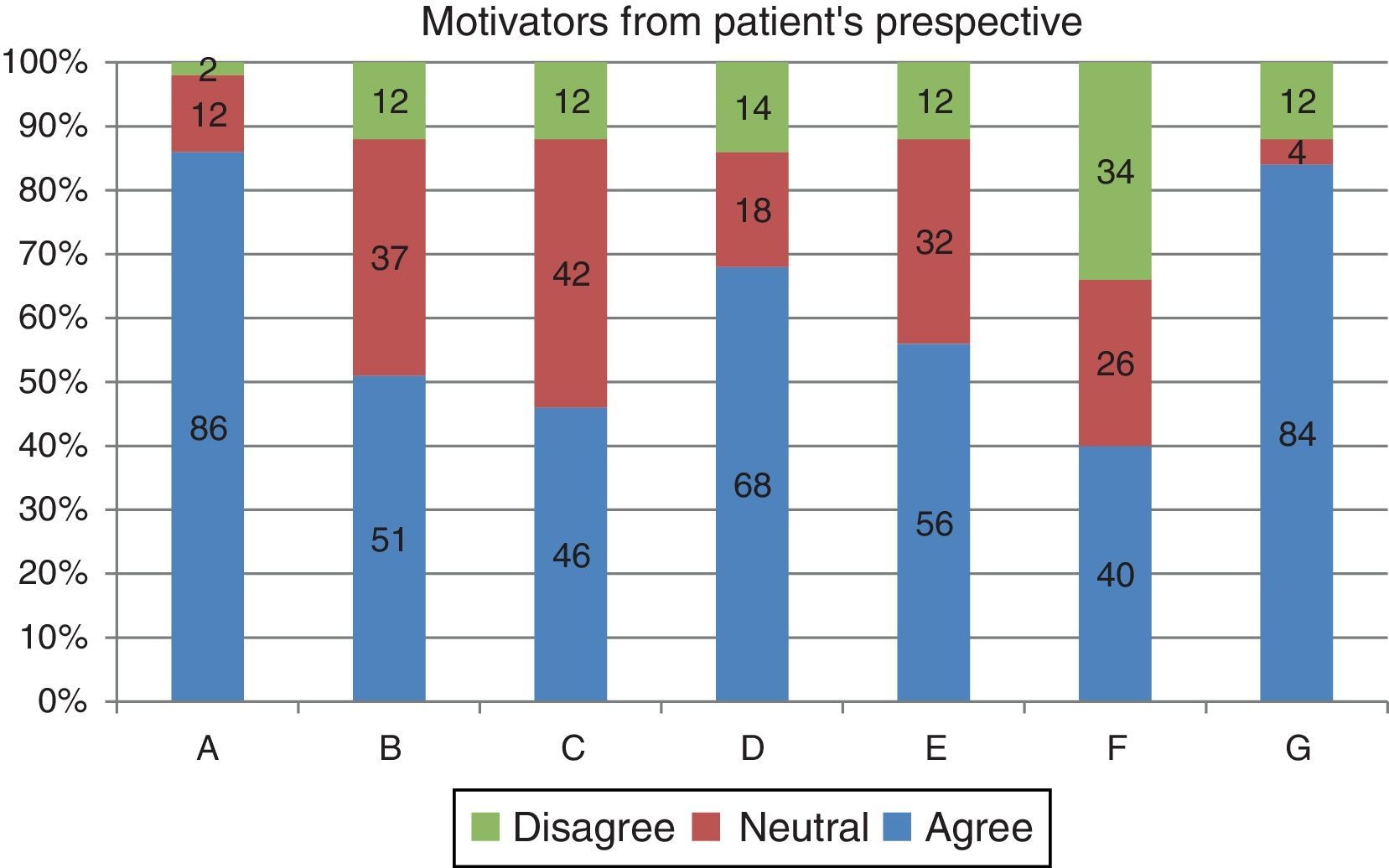
Practitioners who regularly dispensed MFCL reported that professional satisfaction (88%) and better business proposition (82%) were their main motivators in prescribing these lenses (Fig. 4). Availability of the trial lenses (84%) and correct patient selection (82%) enhanced their confidence and worked as major enablers for them (Fig. 5). Natural appearance (86%) and unrestricted field of view (84%) were observed as the major motivators from the patient's point of view (Fig. 6).
 multiple sales and good business proposition, (B) achievement of professional satisfaction, (C) increase in patient loyalty and (D) increase in patient referrals.")
 adequate knowledge and skills, (B) easy motivation through good communication, (C) correct patient selection, (D) increased confidence due to trial lens availability and (E) good awareness through marketing.")
 desired natural look, (B) serves professional requirement, (C) clear vision at all distances, (D) already a CL user, (E) freedom from specific eye and head postures, (F) cost effective as compared to advanced PALs and (G) good field of vision.")
Though graduated optometrist was motivated to dispense MFCL they felt dispensing MFCL did not provide a good business proposition (p=0.02) [B.optom – 73%, D.optom – 93% and Others – 50%] as compared to the diploma holders. Experienced practitioners were found to be least motivated for dispensing these lenses (p=0.01) [experience up to 8.5years-14% and experience >8.5year-54%]. These practitioners strongly believed that their patients found these lenses highly priced (p=0.02) [experience up to 8.5years-32% and experience >8.5year-50%] and thus would not consider using them. Stand-alone practitioners were observed to be more neutral and did not give any agreement or disagreement regarding their opinion about the awareness of these lenses among patients (p<0.05) [stand alone practice-43% and retail chain-11%].
DiscussionAlong with barriers, the study also gathered information about motivators and enablers for dispensing MFCL, which may help in planning strategies to overcome the barriers.
In an earlier study Morgan et al. hypothesized that psychological factors, like, the lack of product awareness, fitting skills, technical know-how and confidence among practitioners could be the primary barriers in fitting MFCL.11 While these barriers featured in our study, they were not found to be the most significant ones. Instead, availability of trial lens, power range and increased chair time were observed to be more significant barriers this could be because the study was conducted in India. When this study was conducted, presbyopic lenses from only two multinational companies (B&L and J&J) were available to the practitioners.
Our findings also differed from the assumptions made by Morgan et al. where11:
- •
Possibility of patients losing faith in the practitioner was considered to be a barrier; on the contrary, in our study patient loyalty and increased referrals were found to be motivators.
- •
It was also thought that unavailability of an ideal MFCL leading to compromised visual performance will make the patients dissatisfied, however according to this study practitioners did not think it to be a significant barrier from patient's perspective.
In India, optometry is not a regulated profession. The contact lens practitioners have different educational backgrounds which are briefly described as follows,13
The degree of Bachelors in optometry is granted after four years of training. An additional two years of post-graduate training in clinical optometry provides a master of optometry.
The other option is a two-year diploma program in optometry which emphasizes refraction and ophthalmic techniques.
The third group is made up of practitioners with no formal optometric training.
Today's presbyopes, especially in the metropolitan cities are observed to be leading an active and diverse lifestyle. They are concerned about health and are equally conscious about their appearance.11,12 It was found that more presbyopes, especially females, as compared to males, opt for wearing lenses supporting the fact that this group is more conscious about cosmesis.11 It is important to make them aware of the existence and advantages of these lenses. As about 62% of the practitioners showed least or neutral response in the level of motivation toward dispensing MFCL, increasing the level of self-motivation of the practitioner is very important for dispensing these lenses as that will positively influence their recommendation to the patient.
Experienced professionals and contact lens manufacturers can conduct educational programs in presbyopic contact lens fitting in order to enhance skills of the practitioners. This will not only help boost the confidence of the practitioners but will also help in reducing the extra chair time which is considered as one of the major barriers by practitioners. Practitioners need to be trained on proper patient selection, an important enabler according to our study, as the success of these lenses has great dependence on correct patient selection.12
Manufacturers need to work on not only spreading awareness among the patients but also promote and regularly update the practitioners about newer products and their advantages. Making trial lenses available could aid in persuading these practitioners to try these lenses. Currently there are very few MFCL options available in India. Thus it is very important for the manufactures to invest more in Indian market and increase the availability of various MFCL designs which are available in global market. Availability of better designs and range of trial lenses with more power options will help in increasing the confidence and motivation level of the practitioners to dispense MFCLs.
This study collected responses from the practitioners only. We relied on practitioners’ understanding of their patients’ views and did not directly reach out to the patients as it was important to get the information from the practitioners regarding the barriers faced by them, leading to limited dispensing of MFCL. This was one limitations of this study. Another one is that it was conducted in Mumbai, India. Different geographical locations may have different factors governing the MFCL dispensing.
Scope of future studyWith the current study giving insights on the factors affecting the limited dispensing of MFCL from a practitioners perspective, further research can directly target the patients to understand their perspective regarding MFCL. This will help in better management of the presbyopic lens wearing population in India.
ConclusionDispensing of MFCLs in India can be enhanced by addressing major barriers such as limitations in power range and lack of awareness of availability of these lenses among CL wearers. Making trial lenses readily available might help to build confidence and motivate practitioners to recommend these lenses. Further research and probing are required to understand lack of motivation among experienced practitioners.
Financial disclosureThis work is conducted without external financial support.
Conflict of interestThe authors have no conflicts of interest to declare.
We acknowledge Bausch+Lomb, India professional services team for their help to reach out to the practitioners across Mumbai, India. Our sincere thanks to Dr. Maninder Setia for his help with the statistical analysis and Judith Flanagan for proof reading the manuscript.
The following are the supplementary data to this article:





