


To identify background chromatic contrast preferred subjectively by patients with age-related macular degeneration (AMD).
MethodsProspective observational case series. Study subjects with AMD were recruited and compared to a control group of study subjects with normal vision. Study subjects were presented with letter size printed sheets of white paper with randomly typed 2M size standard black optotypes. Chromatic contrast was created with colored plastic sheets positioned on top of the black on white printed sheets. The 4 major color hues which were selected for testing were blue, yellow, green and red. Study subjects were required to identify background contrast best preferred for viewing at the end of 4 trial sequences.
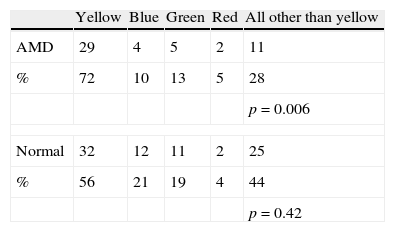
Results40 subjects with AMD were recruited together with 57 study subjects with normal vision. In either the control group or the group with AMD subjects the majority's chromatic preference for background was yellow (56.14%, p=0.42 and 71.67%, p=0.006 respectively) with subjects with AMD preferring yellow color background significantly more than subjects with normal vision (p=0.0002).
ConclusionsYellow color background seems to be preferred by most of healthy and AMD eyes. This preference may be modulated by factors such as the yellow-blue vision processing channel and/or luminosity differences produced by selectively transmitted light.
Identificar el contraste cromático de fondo preferido de modo subjetivo por los pacientes con degeneración macular asociada a la edad (DMAE).
MétodosEstudio prospectivo observacional. Se seleccionó a un grupo de pacientes con DMAE con DMAE para ser comparado con un grupo control de pacientes con visión normal. A ambos grupos de pacientes se les presentaron hojas de papel blanco impresas con optotipos negros estándar de tamaño 2M, en secuencia aleatoria. Se creó contraste cromático mediante láminas de plástico de colores situadas por encima de las hojas impresas en blanco y negro. Se seleccionaron para la prueba los 4 tonos de colores principales: azul, amarillo, verde y rojo. Se solicitó a los pacientes bajo estudio que identificaran el contraste de fondo preferido para la visión, al final de 4 secuencias de prueba.
ResultadosSe seleccionaron 40 pacientes con DMAE, y 57 pacientes con visión normal. Tanto en el grupo de control como en el grupo de pacientes con DMAE la preferencia cromática mayoritaria fue para fondo amarillo (56,14%, p=0,42 y 71,67%, p=0,006 respectivamente), teniendo los pacientes con DMAE una mayor preferencia por el color amarillo que los pacientes con visión normal (p=0,0002).
ConclusionesEl fondo de color amarillo parece ser el preferido por la mayoría de pacientes, tanto sanos como enfermos. Esta preferencia podría modularse mediante factores tales como el canal de procesamiento de la visión amarillo-azul y/o las diferencias de luminosidad producidas por la luz transmitida selectivamente.
Visual perception is a multi-dimensional sense encompassing detection, resolution, recognition and color identification abilities of targets presented for viewing. Visual perception is dependent on detection of hue differences between the target observed and its background. Chromatic contrast facilitates visual perception and chromatic contrast sensitivity seems to be superior to black versus white contrast sensitivity.1 Aside from the psychophysical measures which qualify such abilities, functional vision measures provide the true utility value of such abilities. Subjective chromatic contrast preference is such a functional vision measure affected not only by psychophysics but also by a variety of other factors. Attempts made in the past to relate subjective chromatic contrast preference to objective psychophysical outcome measures did not produce conclusive evidence to support any prescribing protocol of chromatic contrast.2 A logical approach to produce a prescribing protocol for subjective chromatic contrast preference would be to separate the assessment into two parts: assessment of abilities to identify chromaticity of targets against an achromatic background in order to quantify chromatic preference of targets and second, assessment of achromatic targets against various chromatic backgrounds to determine chromatic preference for backgrounds. It is the aim of this study to clarify the above second premise.
MethodsThe study was designed as a prospective non randomized observational case series. Patients were identified prospectively as they presented to one of the clinics run by one of us. We selected for this study subjects with previously diagnosed age-related macular degeneration (AMD) and as a control group, subjects with normal vision.
Inclusion criteria for the subjects with AMD group were documented stable macular disease, low vision in both eyes and best corrected visual acuity (BCVA) of 20/50–20/400 in the better eye (test eye) and older than 45 years of age. Excluded from the study were subjects with cognitive impairment, other retinal disease, color blindness, previous retinal surgery (excluding laser), significant media opacity or contraindications to dilation drops. Inclusion criteria for the group of subjects with normal vision were no significant ocular pathology, BCVA better than 20/50 in the poorer eye and age older than 45 years. Exclusion criteria were similar to the group of subjects with AMD.
Demographic details, refraction and BCVA (with ETDRS – Early Treatment Diabetic Retinopathy Study Charts)3 data were collected for both groups. Contrast sensitivity was assessed with the Contrast Sensitivity Function Test (VCTS) chart.4 Screening for color blindness was done using Ishihara color plates.
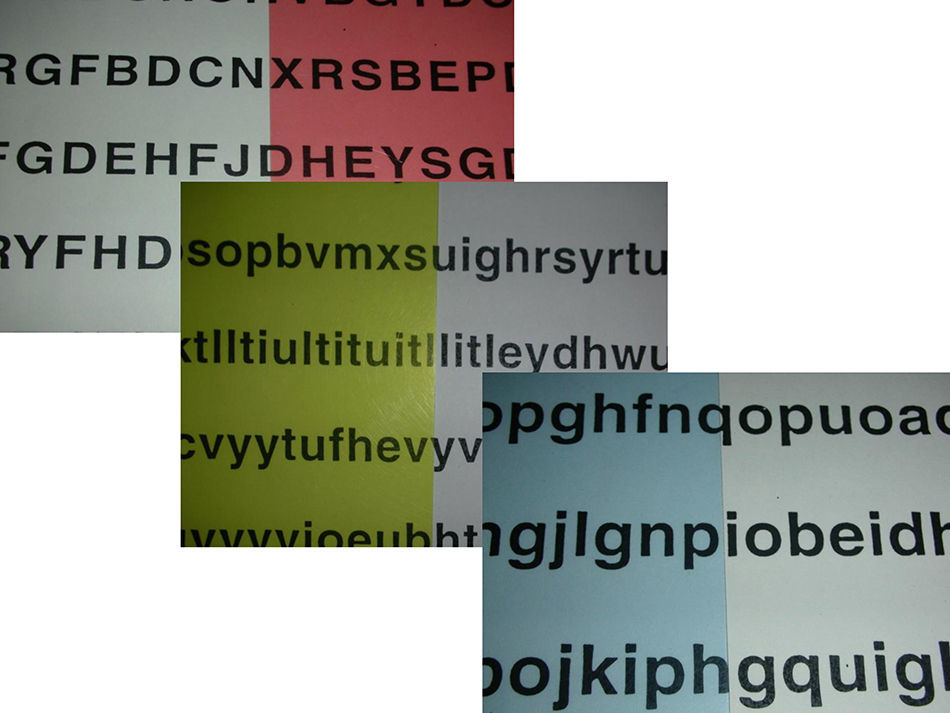
Chromatic contrast was created with colored overlays (www.irlen.com) of plastic sheets positioned on top of the black on white printed sheets (Fig. 1). It was the specific intention of the study protocol to use commercial chromatic sheets widely available from a commercial supplier in order to facilitate duplication of the study. The four major color hues were selected for testing. Blue, yellow, green and red colored overlays were used for testing. Colored overlays were positioned to cover only half of the testing sheet (Fig. 1) and hence creating two distinct side-by-side areas for evaluation of two choices. Colored overlays were presented in a random sequence. Those selecting black over white contrast as preferred over chromatic contrast were excluded from the study. The intent of the study was to test color preference among those who preferred chromatic contrast.

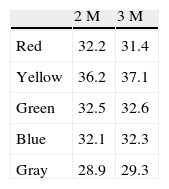
Subjective chromatic preference testing was done in a clinical setting. Normal indoor background illumination was supplemented with a lamp with a 60W frosted incandescent bulb positioned at about 1m from the testing sheet at 45° angle of incidence. This illumination source produced 235 LUX at the testing sheet plane. Viewing distance was allowed to match best correction for near vision available to the subject. Transmission characteristics of the colored overlays were analyzed using an optical lab spectrometer. Transmission curves characteristics for each hue are presented in Fig. 2. Reflectance characteristics of the colored surfaces were measured in a separate experiment. Reflectance was measured using a light meter positioned at 40cm distance from the testing sheet (Table 2).
.")
Each participant, either with normal vision or with AMD was subject to 4 separate experiments. The four testing sequences followed one after another. The first 3 experiments, performed at random, involved choosing a preferred background color out of the 4 options available while viewing a printed 9 “X11” black on white printed sheet half covered with a colored overlay. Each subject had to declare a preference for chromatic contrast against the standard black on white contrast viewed on the other half of the sheet. Subjects were presented with letter size printed sheets of white paper with randomly typed 2M size standard black optotypes in upper case (first experiment), lower case (second experiment) and numerals (third experiment).
Subjects were asked for each experiment to choose which option in their opinion facilitated best reading ability. The question presented each time was “Which color you prefer for reading the characters better?” The choice of color for each testing sequence (upper case, lower case, numerals) was recorded. The color chosen for 2 or 3 of the testing sequences was chosen as representing the color choice of the study subject. Finally the 4th experiment presented on one half of the sheet the background color of choice selected before while the other half of the sheet was covered with a gray overlay. Study subjects were asked to choose the choice of color which provides best reading ability out of the two final choices. The color chosen after the 4th experiment was recorded as representing the final color choice of the study subject.
The primary outcome measure selected for analysis was subjective chromatic background preference. Data analysis was based on descriptive statistics that include frequency distributions, a measure of central tendency (mean) and a measure of dispersion (standard deviation). Statistical comparison between populations was made by Student's t-test for variables meeting the definition for interval measurements. For categorical data analysis we used the binomial and the McNemar tests. Differences were considered to be statistically significant at p value of less than 0.05. The study was performed in adherence to the guidelines of the Declaration of Helsinki. The study protocol was approved by the Research Ethics Committee of the University Health Network of Toronto. Informed consent was obtained from all participants.
ResultsOver a span of about 12 months 40 AMD study subjects (14 males and 26 females) were recruited aged 55–95 years old (mean 79.4 years/SD 8.8). They were compared to a control group of 57 normal vision study subjects (26 males and 31 females) aged 55–95 years old (mean 66.6 years/SD 7.06). The group with normal vision subjects was significantly younger than the AMD group (unpaired t-test, p<0.0001, t=7.9344, df=95, SED=1.613). Mean ETDRS BCVA for the group with normal vision was 0.09±0.1logMar units (20/25) and for the group with AMD was 0.83±0.26logMar units (20/128). The contrast sensitivity measured at 1cyc/degree spatial frequency was poorer in the AMD group than in the group with normal vision (1.00log units, SD 0.58 versus 2.16log units, SD 0.2, respectively) (unpaired t-test, p<0.0001, t=13.99, df=95, SED=0.083). In either the control or AMD group the majority's subjective chromatic preference for background was yellow (56.14%, p=0.006 and 71.67%, p=0.42 respectively, two tail p value with the binomial test). When further comparing paired proportions with the McNemar test between the control group of normal vision subjects and the group of subjects with AMD, the difference between the 2 groups was statistically significant (two tail value, p=0.0002). Blue and green choices for chromatic contrast were more prevalent in subjects with normal vision than in those with AMD (Table 1). There was no difference in contrast sensitivity at 1cyc/degree between those who preferred yellow background and those who preferred other background hues, either in those with normal vision (p=0.5) as in those with AMD (p=0.23).
Subjects with AMD preferred a yellow color background significantly more than subjects with normal vision (p<0.0001). Subjective chromatic preference could be correlated to age in the group with normal vision with other color backgrounds preferred by the younger subjects (less than 67.32±0.33 years) (p=0.0001) and yellow by the older ones. The same could not be shown for the group with AMD cases (p=0.45).
DiscussionEvidence-based practice is the cornerstone of modern medicine. It also applies to low vision rehabilitation (LVR), a relatively new sub-specialty in ophthalmology.5 A leading trend in current research aims to characterize the functional aspects of visual deficits. Unfortunately, the practice of LVR is supported by few evidence-based studies and it is quite frustrating when one contemplates interventions aimed at improving functional vision with chromatic contrast. This is due not only to the paucity of numbers of research papers in LVR but also to the complex nature of color vision.
Psychophysical research has revealed that vision processing operates simultaneously with luminance and chromatic information in processing motion, texture, stereopsis and shape identification.6 Chromatic information seems to be helpful with visual processing at lower spatial frequencies.7 This was confirmed also with low vision patients who lost macular function and visual processing relies mostly on the residual lower spatial frequencies.8 Processing background information is usually the attribute of the peripheral retina processing information mostly via lower spatial frequencies channels. This is possible due to the fact that apparently more cones than rods are spared in macular and paramacular areas in AMD cases.9
Interventions aimed at improving functional vision with chromatic contrast were scrutinized not only in the past but also in the context of low vision rehabilitation. No conclusion could be reached however in a recent major review article with regards to recommendations for using specific colors in the context of certain tasks or in relation to various pathologies.2 Colored overlays were found not to provide a clinically significant improvement in reading rates for people with non-exudative AMD associated with a relative scotoma and central fixation.10 Yet another study found that use of filter lenses may improve contrast sensitivity in patients with AMD.11 Yet another study found that yellow filters may be useful when enhancement of low achromatic contrast is desirable.12
In any given situation when chromatic contrast is assessed, the relationship between the target and the background provides the strongest argument for defining perceptual abilities and is defined as chromatic contrast sensitivity. Yet the independent role of these components from a functional vision point of view was never highlighted in low vision research.
We found that in either the control or AMD groups the majority's subjective chromatic preference for background was yellow. The second choice for all was blue or green. This finding may be in line with the accepted opponent process color theory which states that the human visual system interprets information about color by processing signals from photoreceptors in an antagonistic manner. The opponent color theory suggests that there are three vision perception channels with opponent colors competing for perception: red versus green, blue versus yellow, and black versus white. Responses to one color in one of the channels are antagonistic to the other opponent color. The vast majority of respondents in our study (subjects with normal vision 77%, those with AMD 85%) selected the yellow-blue channel colors as the ones defining best chromatic background preference, against green-red channel colors (normals 23%, AMD 15%).
This relationship between any chromatic target and its chromatic background is modulated also by luminance. Luminance is an independent factor which also may have affected the results of this study. This factor was also an item of study in our research design for this project. In our design we limited ourselves to provide standard external illumination which is standard for viewing visual acuity charts at 1m distance in a standard clinical testing facility in an uniform way throughout the testing sessions.
The obvious common observation was that yellow background by virtue of being a lighter color than the others tested reflects back more light and hence has a larger contrast impact for any target viewed against it. This is confirmed and detailed in the reflectance data summarized in Table 2. Looking however at the transmission curves of the hues used, one can deduce that luminance was indeed a major factor in the selection of the hue of choice. Yellow and green overlays allowed light transmission in the mid-range more than the other hues tested. Yellow overlays in addition to higher transmission in the mid-range spectrum also blocked most effectively transmission in the low range spectrum. This last aspect reduced the component of glare significantly.
An additional significant finding from our study is that subjects with AMD preferred yellow background more than those with normal vision. The highly significant statistical value (p=0.0002) suggests that indeed the variable defined as AMD pathology may be responsible for this outcome.
Background chromatic preference seems to be modulated via several mechanisms. It is not clear from our study which one has more weight but all seem to indicate a preference for yellow color background. To the best of our knowledge this was never reported in the literature.
This study was designed as a pilot study. The main limitation of this study is that it was designed and implemented in a clinical setting rather than in a laboratory. Results present data only from exploration of the first part of our research postulate, the preference of chromatic background. Further studies hence, with more stringent criteria are required in order to validate the concepts advanced in this paper.
The main benefit derived from our study is that it brings a measure of logic in the complex practice of functional chromatic LVR. It offers evidence that yellow hues are perhaps the most useful as background contrast in various task related situations and this knowledge can be applied and tested immediately in clinical practice. We hope that these suggestions will serve base for other studies to follow which will clarify further issues raised by us in this paper.
Conflicts of interestPresented at Research Day, Department of Ophthalmology and Vision Sciences, University of Toronto, Ontario, Canada, May 9, 2008.
The authors have no conflicts of interest to declare.





