






Spectral filters have been used clinically in patients with mild traumatic brain injury (mTBI). However, they have not been formally assessed using objective techniques in this population. Thus, the aim of the present pilot study was to determine the effect of spectral filters on reading performance and visuo-cortical responsivity in adults with mTBI.
Methods12 adults with mTBI/concussion were tested. All reported photosensitivity and reading problems. They were compared to 12 visually-normal, asymptomatic adults. There were several test conditions: three luminance-matched control filters (gray neutral density, blue, and red), the patient-selected ‘precision tint lens’ that provided the most comfort and clarity of text using the Intuitive Colorimeter System, and baseline without any filters. The Visagraph was used to assess reading eye movements and reading speed objectively with each filter. In addition, both the amplitude and latency of the visual-evoked potential (VEP) were assessed with the same filters.
ResultsThere were few significant group differences in either the reading-related parameters or VEP latency for any of the test filter conditions. Subjective improvements were noted in most with mTBI (11/12).
ConclusionsThe majority of patients with mTBI chose a tinted filter that resulted in increased visual comfort. While significant findings based on the objective testing were found for some conditions, the subjective results suggest that precision tints should be considered as an adjunctive treatment in patients with mTBI and photosensitivity.
Los filtros espectrales han sido utilizados clínicamente en pacientes con lesión cerebral traumática leve (mTBI). Sin embargo, no han sido evaluados formalmente utilizando técnicas objetivas en esta población. Por tanto, el objetivo del presente estudio piloto fue el de determinar el efecto de dichos filtros sobre el rendimiento lector y la respuesta visual-cortical en adultos con mTBI.
MétodosSe realizaron pruebas a doce adultos con mTBI/conmoción. Todos ellos reportaron fotosensibilidad y problemas lectores. Se realizó una comparación con adultos asintomáticos y con visión normal. Las pruebas se llevaron a cabo bajo diversas situaciones: uso de tres filtros de control con equivalencia de luminosidad (gris con densidad neutra, azul, y rojo), ‘lentes tintadas de precisión’, seleccionadas por el paciente, que aportaban mayor confort y claridad de texto utilizando un sistema colorimétrico intuitivo, y valores basales sin utilizar ningún filtro. Se utilizó el Visagraph para evaluar los movimientos oculares durante la lectura y la velocidad lectora de manera objetiva con cada filtro. Además, se evaluaron tanto la amplitud como la latencia de los potenciales evocados visuales (VEP) con los mismos filtros.
ResultadosSe produjeron pocas diferencias grupales significativas, tanto en relación a los parámetros relacionados con la lectura como a la latencia de los VEP, en cualquiera de las situaciones de prueba de los filtros. Se notaron mejoras subjetivas en la mayoría de sujetos con mTBI (11/12).
ConclusionesLa mayoría de los pacientes con mTBI eligieron un filtro coloreado que incrementó su confort visual. Aunque se detectaron hallazgos significativos basados en las pruebas objetivas para algunas situaciones, los resultados subjetivos sugieren que deben considerarse las lentes tintadas de precisión como tratamiento adyuvante en los pacientes con mTBI y fotosensibilidad.
The omnipresence of printed material and computer-based technology in modern society has made reading a fundamental skill for both professional success and daily functioning. Thus, those with reading dysfunctions have difficulties in both career and non-career related milieus.1 Individuals with mild-traumatic brain injury (mTBI) are one such population in whom post-injury visual sequelae often result in a significant reading disability, with most (up to 90%) reporting to have a ‘reading problem’.2 The etiology of the reported reading problems is likely multifaceted: approximately 90% of those with mTBI and vision-related symptoms have an oculomotor dysfunction,3 10–40% have accommodative deficiencies,3,4 and 50% report some degree of light sensitivity.5 Reading is uniquely affected by deficits in each area. For example, oculomotor dysfunction affects fine binocular oculomotor coordination as one scans across a line of text,1,6 accommodative dysfunction alters textual clarity,3 and light sensitivity limits comfort and one's maximum reading duration.5 Re-integration into daily life in these afflicted individuals is hindered by such reading disabilities. Thus, optimal treatment necessitates therapies which provide long-term symptomatic relief in all three areas.
Band-pass spectral lenses (i.e., ‘colored filters’) are one possible treatment: how could they address each symptom? Colored filters alter the spectral composition and reduce the luminance of the incoming light.4,8 Changes in spectral composition alter the locus of the retinal light bundle: blue light is focused myopically, and red light is focused hyperopically. Thus, filters which primarily transmit blue light decrease the accommodative demand9: this may provide some degree of symptomatic relief for those with accommodative insufficiency.10 The resultant increased accommodative accuracy may have a positive effect on both accommodative convergence and convergent accommodation and their interaction, which in turn, impacts upon and improves overall oculomotor control and clarity during the complex task of reading at near.1 On the other hand, luminance reduction contributes to an overall reduction in light intensity at each wavelength; accordingly, neutral gray filters are often used to increase visual comfort in those with photosensitivity/photophobia.11,12 Thus, treatment of reading disabilities with spectral lenses has the potential to remediate, or reduce, all three visual symptoms frequently associated with mTBI. The effects of altering spectral composition and luminance of the retinal light bundle on oculomotor function are the primary subjects of the current study.
The present investigation is the first to use objective eye movement recordings to directly assess the effect of colored lenses on reading-based oculomotor function: all prior studies have used indirect measures, such as subjectively-based reading rate. Nonetheless, beneficial effects have been noted in several clinical populations: visually-symptomatic students prefer to read with chromatic filters which reduce the accommodative demand,10 colored filters increase oral reading rate in stroke,13 and colored lenses improved both contrast sensitivity and oral reading rate in those with acquired brain injury.14 Patients with macular degeneration also experience increased contrast sensitivity when wearing colored lenses; however, this effect is limited to the yellow-orange region of the visible spectrum.15 Conversely, the use of colored filters in visually-normal individuals has yielded equivocal results: asymptomatic students prefer to read with filters which do not change the accommodative demand,10 and the use of either band-pass or neutral density gray filters has been shown to increase error rate in visually-normal individuals as compared to reading without any filter.16
The current pilot study aimed to address knowledge gaps in the aforementioned areas. First, as mentioned previously, the objectively measured effects of spectral modification on specific reading-related oculomotor parameters remain largely unexplored. The aforementioned investigations are informative, but they do not provide a proxy for direct assessment of oculomotor performance. Specifically, oral reading rate is reflective of the output of many systems (e.g., attention, comprehension, oculo- and facio-motor effects). Thus, we aimed to use objective eye movement recordings and silent reading to assess the effect of spectral lenses on reading rate and reading-related oculomotor performance. Second, prior investigations used either specific bandwidths10,15 or allowed each subject to choose his or her ‘optimal’ tint through iterative procedures aimed to minimize visuoperceptutal distortions.10,14 To disambiguate the effect of wavelength and luminance reduction, we used specific spectral bandwidths that were individually chosen, as well as pre-chosen spectral and neutral density filters, in our experimental design. Last, we aimed to measure reading performance of both the visually-normal and mTBI populations when these filters were worn for comparative purposes.
Thus, the primary goal of the current investigation was to determine if and how spectral modification affects oculomotor performance and reading. In addition, effects of the different filters were assessed using the visual-evoked potential (VEP)16,17 as a complement to a prior investigation in our laboratory, which measured VEP responses while visually-normal individuals wore spectral lenses.8 Human electrophysiological studies which have documented correlated, positive changes in cortical responsivity (e.g., fMRI,18 steady-state VEP19) while light-sensitive patients wore spectral filters also motivated the inclusion of the VEP technique.
Our hypothesis was that the precision tint would optimize reading performance and/or visual-cortical activity, as well as produce improved visual comfort.
Materials and methodsSubjectsTwelve, visually-normal individuals (7 females and 5 males) with a mean age of 23.3 years (SD±1.4, range 21–26 years), were recruited from the students and faculty at SUNY State College of Optometry. Subjects with a history of seizures, or the presence of strabismus, amblyopia, ocular or systemic disease, and/or neurological disease were excluded. Individuals had corrected visual acuity of 20/20 or better, both binocularly and monocularly, at distance and near. Each had normal contrast sensitivity.20 Mean spherical refractive error was −2.75D, with a range from +1.25D to −6.25D. Mean astigmatism was −1.18D, with a range from plano to −2.75D.
Twelve subjects (10 females and 2 males) with concussion/mTBI were recruited from the University Eye Center, as well as from the students and faculty at SUNY College of Optometry. They had a mean age of 35.07 years (SD±13.43, range 21–60 years). There was not a significant difference in ages between the two groups (t-test p>0.05). Their concussion/mTBI was caused by either a sports-related injury (n=6), motor vehicle accident (n=2), or other traumatic event (n=4). Subjects were past the natural recovery period of 6–9 months21 post-injury, as the trauma occurred within a time period of 1-0 years (mean=4.97 years) prior to our laboratory testing. The following criteria were used for the diagnosis of mTBI21: (1) loss of consciousness for less than 30min or an altered state of consciousness, (2) post-traumatic amnesia (PTA) lasting less than 24h, and (3) Glasgow Coma Scale score of 13–15. This was determined per their medical records and/or self-reported detailed history. All subjects had corrected visual acuity of 20/20 or better both binocularly and monocularly at distance and near, with normal contrast sensitivity.20 Mean refractive error was −1.00D, with a range from +1.00D to −4.75D. Mean astigmatism was −0.39D. Subjects with a history of seizures, cognitive dysfunction, strabismus, amblyopia, ocular or systemic disease, and/or any degenerative neurological disease, were excluded. All had the symptom of photosensitivity by self reporting, following their head injury and at the time of testing; pre-injury prevalence of their photosensitivity was unknown.
Written informed consent was obtained from each subject prior to commencement of the experiment. The study was approved by the IRB at the SUNY College of Optometry.
ApparatusVEP systemThe DIOPSYS™ NOVA-TR VEP system (Diopsys, Inc., Pine Brook, NJ, USA) was used to present a central, full-field (17°H×15°V), alternating, black-and-white, checkerboard pattern stimulus (64×64, equivalent to 20min arc or Snellen acuity of 20/264 at 1m). The mean Michelson contrast was 87% for all test conditions. The visual stimulus was viewed binocularly with both the full refractive correction and each band-pass chromatic test filter in place at a viewing distance of 1m. The baseline stimulus luminance was 74cd/m2. Test duration was 20s per trial.16
Signals were obtained from three Grass gold cup scalp electrodes (Grass Technologies, Astro-Med, Inc., West Warwick, RI, USA). They were 1cm in diameter and consisted of a ground, reference, and active electrode. The sampling rate was 1024Hz, and an amplification factor of 10,000 was used. This system has been used in our VEP brain injury laboratory for over 5 years for several experiments.22 The electrophysiological parameters that were recorded for each of the 5 test lens conditions included the VEP amplitude and VEP latency.
Visagraph systemThe VISAGRAPH™ II system (Taylor Associates, Huntington, NY) is a specialized infrared, computer-based, horizontal eye movement recording system that has been developed for objectively-based reading assessment using standardized graded text. The Visagraph II system provides computer recorded, graphically displayed, and objective reading eye movements with automated analysis.23
The following parameters were assessed: number of regressions per 100 words, number of fixations per 100 words, fixation duration (ms), and reading rate (words per minute, wpm) for each of the 5 test conditions. Reading material was comprised of a single paragraph, being a 100 words story that was standardized for 10th grade reading level.24 The paragraphs subtended 20° horizontally and 10° vertically, and they were comprised of high contrast (90%) 20/50 letters.
Signals were obtained from the Visagraph infrared goggles that tracked the subject's binocular, horizontal eye movements. Resolution is better than 1°. The goggles were held in place with an adjustable band and were fit per the manufacturer's instructions.
Band-pass chromatic (BPC) filters and viewing spectaclesThree standard spectral filters, which altered the incident wavelength spectrum and reduced luminance, were used. The lenses and their wavelengths of peak transmission were: gray/neutral density (uniform transmission), blue (425nm), and red (650nm). These lenses were chosen from the Intuitive Colorimeter system18,25 (Fig. 1). The blue and red lenses were specifically chosen to probe two distinct bandwidths of the visual spectrum (i.e., short and long-wavelengths, respectively). The standard gray lenses (i.e., neutral density-type filters) were used as a wavelength independent control. Red, blue, and neutral density filters are frequently prescribed clinically for special populations, such as to patients with TBI to reduce their visual symptoms, including photosensitivity, glare, and other visual disturbances,5,7 as well as to improve global reading ability and visual comfort.14,26 In addition to the above 3 filter lenses, a subject-specific “precision tint lens” (PT), which the subject chose based on personal maximal comfort and clarity while viewing text in the Intuitive Colorimeter System, was also used. The Intuitive Colorimeter system allows the patient to subjectively select the optimal hue and saturation, as well as luminance combination, that reduces their light sensitivity, minimizes perceived distortions of the text, and/or improves reading efficiency, and it has been used in a range of diagnostic groups (e.g., visual stress,19 stroke,14 mTBI7). Lastly, there was a baseline condition without any filters in place over their spectacle correction.
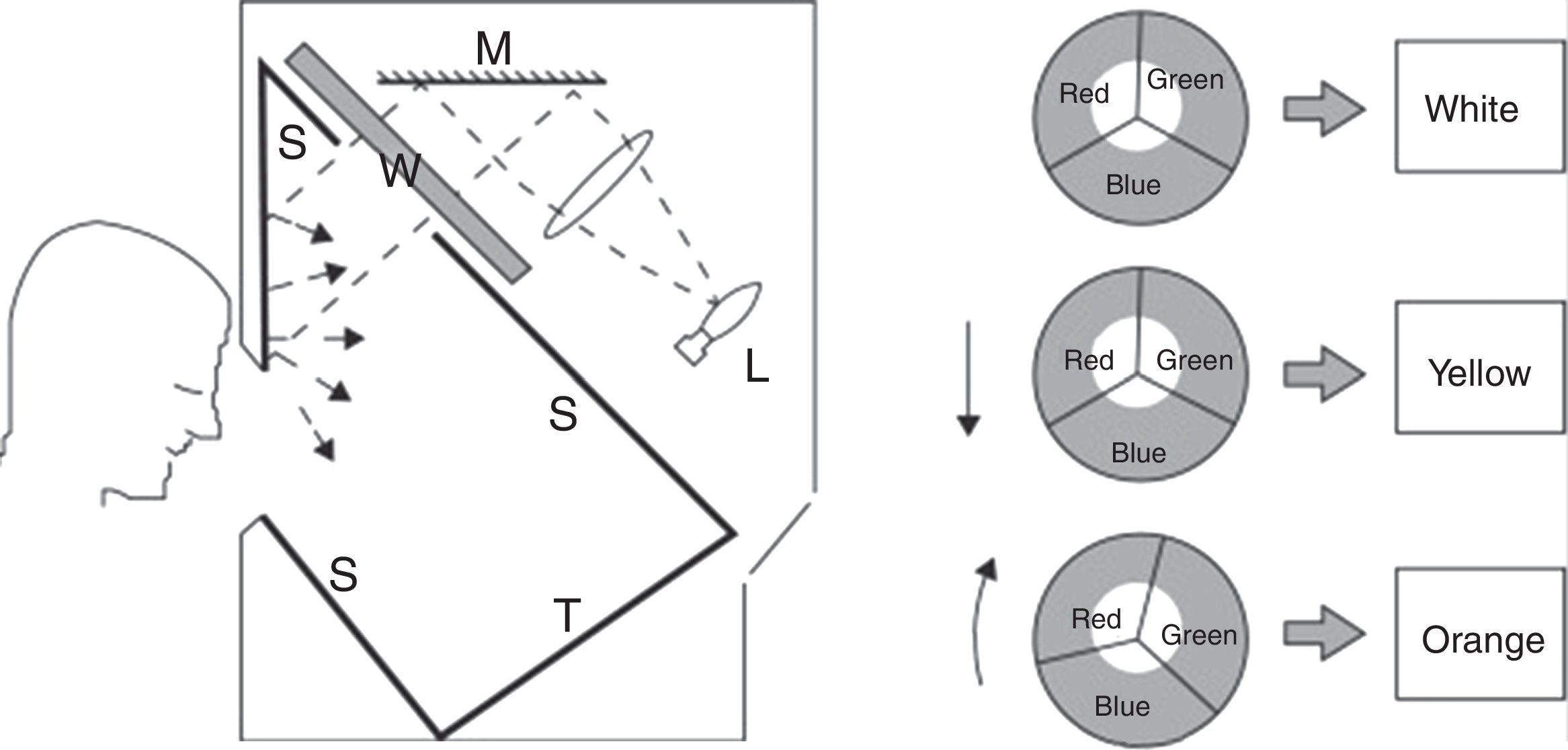
Cross-sectional view of the Intuitive Colorimeter. A beam of white light from a tungsten halogen lamp (L) is reflected from a mirror (M) and passes through a wheel (W) and into a box with matte white inner surfaces (S). The wheel is divided into three sectors, each covered with a different filter so as to transmit light of a different color (red, green, or blue). The colored light is mixed as it is reflected and scattered from the inner surfaces of the box. Calibrated text (T) is mounted on one surface of this box and viewed through a window in the front. Viewing distance is approximately 40cm (2.5D). Saturation increases with eccentricity of the white beam, whereas hue changes with rotation.
Each test filter was 70mm in diameter. To assemble the test spectacles (Fig. 2), each filter (or filter combination, as required to achieve the desired spectral transmission curve), was placed into a black spectacle holder provided by the Intuitive Colorimeter System. Separate test spectacles were configured for each filter. See Willeford et al.,8 for the spectral transmission curves. Each lens had a transmission of 39% in the visible spectrum (400–700nm), as measured with the OptiSource Multimeter Spectrophotometer (OptiSource International, Bellport, NY). The effective mean screen luminance was 29cd/m2 with the filters in place, as was measured with the PR-524 Litemate (Photo Research, Incorporated, Chatsworth, CA).
ProceduresVisagraphInstructions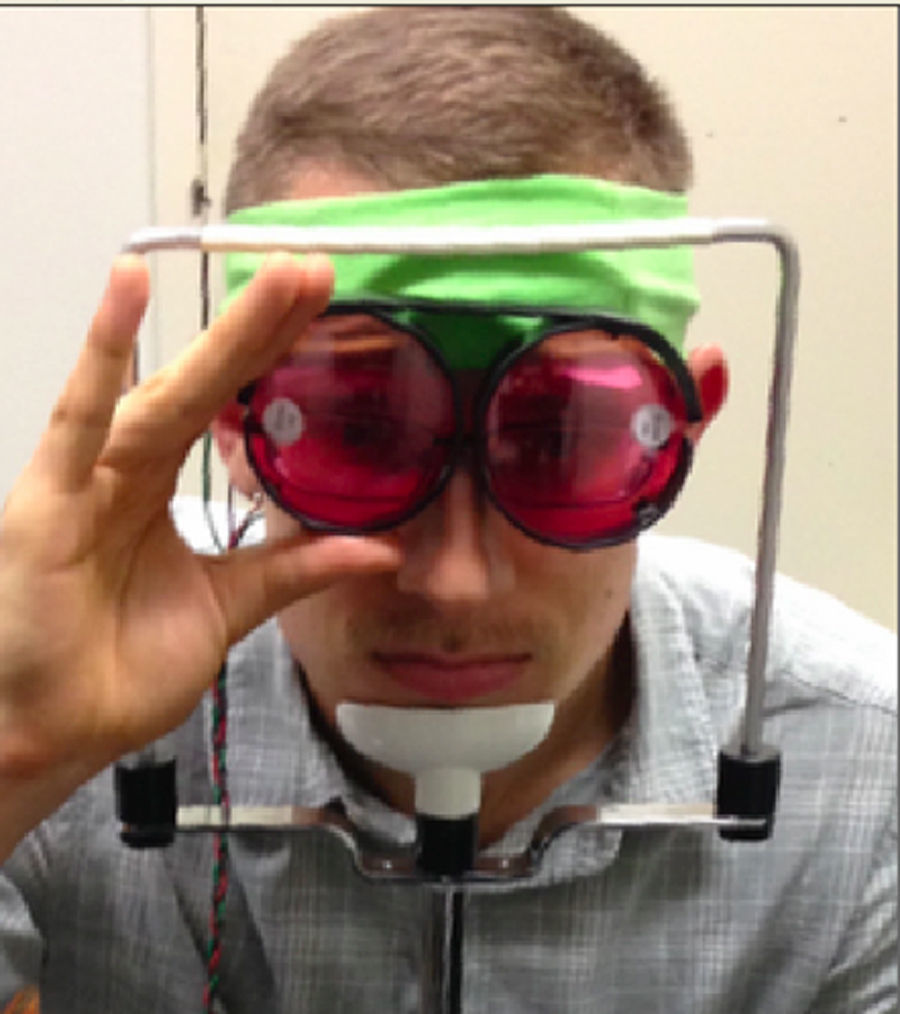
Subjects were instructed to sit in front of the initially occluded reading material, which was centered along the midline, with their eyes leveled with the reference point located above the covered paragraph. The subject was asked to place their chin into an adjustable floor-mounted, headrest/chinrest assembly that was positioned 40cm from the reading material to ensure that there was no excess head movement, and furthermore that only eye movements were used while reading the paragraphs. The Visagraph goggles were placed on and held snuggly with an adjustable band. The pupils were aligned in the goggles per the manufacture's instruction to ensure accurate responses. The cover was removed, and a practice trial was conducted on each subject prior to testing to ensure that adequate eye movements were recorded, and furthermore, that they understood and could perform the test.
TrialsFive trials were conducted with either the red (R), blue (B), neutral density (ND), or the precision tint (PT) lenses, as well as the “eyes open”, or no lens (NL), condition. Reading paragraph sequence was administered in the same order for every subject, while the filter condition was introduced in a random order for every subject to minimize an order effect. Different paragraphs were used for each test filter conditions. All subjects were tested with adult level 10 reading material, with each paragraph having 100 words. Subjects were instructed to maintain head alignment during the procedure and to only move their eyes while reading. After each short paragraph, the subject answered 10 true/false questions to assess their level of comprehension. A minimum score of 70% was required to ensure proper comprehension of the reading material.
VEP systemElectrode placementThis has been described in detail elsewhere and earlier in the text.22 Impedance of the electrodes was maintained below 5kΩ, per the standards of the International Society for Clinical Electrophysiology of Vision (ISCEV).17
InstructionsSubjects were instructed to sit in front of the test screen, which was centered along the midline, with their chin supported by an adjustable floor-mounted, headrest/chinrest assembly that was positioned 1m from the test screen. They received instructions to maintain fixation on a small (0.5° diameter), red, rotating circle that was in the center of the test screen that controlled for accuracy of fixation and accommodation, which was part of the manufacturer's test software. Subjects were instructed to blink approximately every 5s to reduce the number of artifacts registered by the system that may occur with uncontrollable blinking.22 Any trial with greater than 5 artifacts was discarded.22 To ensure that subjects maintained their attention and alertness, they were informed when the trial was half completed, and when there was 5s remaining.27
TrialsFour trials were conducted for each test condition. The three BPC filters, the PT lens, and the “eyes open” or NL condition, were introduced in a random order. All subjects produced responses which were within normal limits for our laboratory.16,22
Data analysisVisagraphThe number of fixations per 100 words, regressions per 100 words, mean fixation duration, reading rate, and comprehension level were recorded for each of the test lens conditions for each subject using the Visagraph. The group average was determined for each parameter. The group mean values±1 SEM were analyzed for each parameter, lens condition, and group.
A two-way, ANOVA statistical analysis was performed using MATLAB, R2015a (Mathworks, Natick, MA) for the factors of filter condition and group to determine the effect of each spectral lens on the reading parameters between the two diagnostic groups. A p-value of p≤0.05 was considered to be statistically significant.
VEPThe VEP amplitude and latency were recorded for each of the lens test conditions for each subject with the VEP Diopsys System. For each condition, the trial value that either exceeded 1 SD from the mean of the trials, or was the most deviant one, was deleted for that subject to control for outlier effects.28 Both the mean and standard deviation of the remaining trials within each test condition for each subject were stored. The mean amplitude and latency values were calculated for each subject. Then, the group average was determined for each parameter and lens condition.
A two-way, ANOVA statistical analysis was performed using the aforementioned MATLAB program for the factors of filter condition and group to determine the effect of each spectral lens on both the VEP amplitude and latency between the two diagnostic groups. A p-value of p≤0.05 was considered to be statistically significant.
ResultsThe comparative group findings for the six test parameters for each filter condition are presented in Table 1:
- 1.
Number of fixations: There was no effect of filter type. Those with mTBI made significantly more fixations than the normals.
- 2.
Number of regressions: There was no effect on filter type. Those with mTBI made significantly more regressions than the normals.
- 3.
Fixation duration: There was no effect on filter type. Those with mTBI made significantly shorter fixation durations than the normals.
- 4.
Reading rate: There were significant differences in reading rate between the two groups for the different filters. There was a difference between the normals with the blue and the red filters, and those with mTBI using either the red, neutral density or precision tint filters; in each case, the normals read significantly faster than those with mTBI.
- 5.
VEP amplitude: There was no effect of either filter type or group.
- 6.
VEP latency: There was no effect of either filter type or group.
Summary of primary test findings.
| Parameter | Lens condition | Mean parameter value | Mean parameter value |
|---|---|---|---|
| VN | TBI | ||
| Reading rate | NL | 247.60 | 192.66 |
| ND | 263.55 | 178.16 | |
| B | 282.70 | 187.08 | |
| PT | 257.20 | 171.81 | |
| R | 282.90 | 171.83 | |
| Number of fixations | NL | 71.25 | 119.50 |
| ND | 72.90 | 121.41 | |
| B | 60.41 | 119.00 | |
| PT | 69.66 | 126.00 | |
| R | 67.33 | 133.91 | |
| Number of regressions | NL | 10.33 | 18.66 |
| ND | 8.55 | 21.25 | |
| B | 7.08 | 19.41 | |
| PT | 8.16 | 19.09 | |
| R | 7.50 | 17.91 | |
| Fixation duration | NL | 355.50 | 300.00 |
| ND | 396.36 | 305.83 | |
| B | 367.50 | 305.83 | |
| PT | 362.50 | 316.36 | |
| R | 383.33 | 303.33 | |
| VEP AMP | NL | 13.63 | 15.27 |
| ND | 13.09 | 16.08 | |
| B | 13.36 | 14.33 | |
| R | 13.66 | 13.91 | |
| PT | 13.72 | 14.86 | |
| VEP latency | NL | 109.12 | 107.67 |
| ND | 111.63 | 113.39 | |
| B | 112.14 | 112.32 | |
| R | 111.94 | 111.25 | |
| PT | 110.88 | 112.41 | |
The individual subject findings for each group and filter type for both reading rate and VEP amplitude are presented in Table 2. There were no consistent trends. With respect to reading rate in those with mTBI: 4 read best with no filter, 3 read best with the neutral density filter, 2 read best with the blue filter, 2 read best with the precision tint, and 1 read best with the red filter. There was no clear relation between filter performance and either reading rate or largest VEP amplitude in the mTBI group. Interestingly, 6 read best with the blue filter in the normal group. Again, there was no clear relationship between filter performance and either reading rate or largest VEP amplitude in the normal group.
Spectral filtered used that resulted in the best and worst results in each VN and mTBI subject for the two parameters (i.e. RR=reading rate and VEP Amp=VEP amplitude).
| Subject | Best | Worst | ||
|---|---|---|---|---|
| R.R. | VEP AMP | R.R. | VEP AMP | |
| N1 | NL | R | ND | NL |
| N2 | B | NL | NL | R |
| N3 | B | NL | ND | ND |
| N4 | B | NL | NL | B |
| N5 | ND | PT | B | NL |
| N6 | ND | PT | NL | ND |
| N7 | NL | NL | ND | PT |
| N8 | ND | R | NL | ND |
| N9 | B | B | NL | PT |
| N10 | NL | PT | R | ND |
| N11 | B | B | PT | PT |
| N12 | B | R | ND | NL |
| TBI1 | ND | NL | PT | PT |
| TBI2 | R | R | ND | NL |
| TBI3 | ND | ND | R | R |
| TBI4 | NL | ND | ND | PT |
| TBI5 | NL | ND | ND | B |
| TNI6 | B | B | NL | PT |
| TBI7 | PT | ND | R | B |
| TBI8 | PT | ND | R | R |
| TBI9 | NL | ND | ND | PT |
| TBI10 | NL | * | ND | * |
| TBI11 | ND | * | R | * |
| TBI12 | B | NL | R | B |
We questioned whether wearing specific spectral filters could improve reading-related oculomotor performance. There were few significant differences found in any of the reading-related oculomotor parameters when comparing any of the filters to the NL condition within either group. Thus, neither of the two proposed mechanisms (i.e., altered spectral composition or luminance reduction) seems to alter oculomotor performance during reading consistently in either the mTBI or visually-normal populations, at least during the short test periods. There was no correlation between a subject's chosen PT and the filter with which he or she performed best.
The effect of spectral filters on the VEP parameters was also similar in the two populations studied. First, each filter increased the VEP latency as compared to the baseline, NL condition. A prior investigation8 suggested that approximately 75% of the effect on latency can be attributed to the decrease in overall luminance, with the remaining 25% of the effect due to differences in chromatic processing speed. Second, the lenses had no effect on the VEP amplitude: this is contrary to what was found by Riddell et al.,20 who reported increases in steady-state VEP amplitude while each subject wore his or her precision tint. The plausible reason for this difference might be that the Riddell et al. used steady-state VEP, not the transient VEP, as used in the current study.
The VEP system measures the “middle-early” stages of visual processing, and the neural activity in the visual cortex, in response to a time-locked visual stimulus.17 The main response seen in the VEP system is primarily activated by cone photoreceptors in the central 15° of the visual field,17,22,29 which corresponds to approximately 50% of the primary visual cortex (i.e., cortical magnification factor).22,30 However, if the beneficial effect of the spectral lenses occurs either at the initial stages of visual processing, such as on accommodation,10 or at a later stage of processing, i.e., past V1, its effects may therefore not necessarily be recordable using VEP technology. If the chromatic lenses do effect, and possibly enhance, the later stages of visual processing, this could explain the subjective increase in visual comfort reported by the majority of the subjects, despite no improvement on the VEP parameters measured, as found in the present investigation.
Despite similar objective findings while subjects wore the different spectral filters, a majority of the mTBI population selected a PT. Like many holistic solutions, it may be the subjective appreciation of visual comfort that psychologically helps, but is neither statistically significant nor recordable with the present instrumentation. In fact, the equiluminance of each test filter suggests that the reduction in overall luminance may be the key factor to provide increased visual comfort to photosensitive patients while reading, regardless of the spectral composition of the light.
The results from our investigation are reminiscent of the vast literature regarding the clinical use of colored lenses. Specifically, while several studies have documented objective correlates of improved functionality (e.g., improved contrast sensitivity in patients with TBI,14 AMD15), an equivalent number of reports have found objective correlates with unclear functional benefits (e.g., improved ss-VEP amplitude in children with visual stress20) or functional benefits without objective correlates (e.g., reduced symptomatology). The elucidation of a strong link between objective measurements and functional benefits is hindered by two sources of variability: internal (i.e., within a patient) and external (i.e., in the environment). First, the clinical conditions in which spectral lenses are primarily used (e.g., retinal dystrophies and degenerations, TBI) exhibit a large degree of variability in presentation and progression. Thus, given the heterogeneous retinal and cortical architectures present in such populations, the effect of a spectral lens may be dependent on each individual's anatomical and physiological state. Second, the spectral composition of the world itself is infinitely diverse. The comparison of results across studies necessitates equivalent test conditions (e.g., equiluminant black text on white backgrounds); similarly, it is imperative for clinicians to demonstrate the effects a spectral prescription may have in different lighting environments prior to dispensing.
ConclusionsTherefore, based on the results found in this pilot study, the use of tinted lenses as a mechanism to increase comfort in those with mild traumatic brain injury would be a reasonable first step prior to initiation of further rehabilitative therapies (e.g., vision therapy).31 These additional therapies can more directly treat the underlying oculomotor dysfunctions common in those with concussions and mild traumatic brain injuries. Tinted lenses may be a viable solution to relieve initial discomfort in this population before a longer-term resolution (e.g., vision therapy) is implemented.
Study limitationsThere were two possible study limitations. First, sample size was small; however, it was not inappropriate for a pilot study. Second, subjects only wore each filter for a few minutes during the reading assessment, as is typically done in such studies. They should be assessed with each lens initially, and then with at least the PT and the control neutral density filter, in a counterbalanced manner over a period of hours/weeks/months to determine if there are any beneficial effects/visual adaptations that might occur over the short- and long-term both with respect to visual comfort and reading efficiency. Lastly, we did not measure each subject's reading rate or VEP amplitude with a green filter, therefore our results do not include the effect the central color spectrum would have on our measured parameters in this experiment.
Future directionsThere are several possible future directions for study, as this was a pilot investigation. First, it should include a much larger sample size (e.g., 50–100) to test for generality of any phenomenon/trends and possible subgroup effects. Second, follow-up assessments should be performed over an extended time course (e.g., 6–12 months) with respect to visual comfort and reading ability with the precision filter, and perhaps also the neutral density control filter. Third, other naturalistic/real-life tasks should be assessed with the filters, such as ambulating, driving, computer work, near visuomotor activity, etc. Fourth, detailed testing might include other diagnostic groups, such as those with migraine, stroke, dyslexia,32 etc. And, lastly, brain imaging should be performed at the various test stages to determine what neural areas may be involved in the overall process and phenomenon.
Conflicts of interestThe authors have no conflicts of interest to declare.
We would like to thank Cerium Visual Technologies for the loan of the Intuitive Colorimeter, and Diopsys for the loan of the VEP system.





