

To investigate the natural change of nearwork-induced transient myopia (NITM), and its association with the progression of refractive error.
MethodsStudents of the Beijing Myopia Progression Study were examined at baseline and follow-up examinations, which included cycloplegic autorefraction. Initial NITM and its decay were assessed objectively immediately after binocularly-viewing and performing a sustained 5-minute near task (20 cm).
ResultsThere were 223 students with both NITM and cycloplegic refractive data enrolled. There were 142 myopic (63.7%), 32 emmetropic (14.4%), and 49 hyperopic (22.0%) students according to their baseline cycloplegic refraction. The annual refractive change was −0.45 (−0.73, −0.21) D. From the baseline to the one-year and two-year follow-up periods, the initial NITM (median) increased significantly in the myopic students (0.16, 0.21, and 0.20D, p = 0.01, respectively). The overall proportion of NITM decay types shifted significantly from none being induced at baseline (non-induced: 17.0%, complete decay 57.4%, incomplete decay 25.6%) to incomplete decay at the 2-year follow-up (non-induced: 6.7%, complete decay 65.0%, incomplete decay 28.3%, p = 0.01). For the hyperopic students, after adjusting for risk factors, for every 1 diopter increase in the initial NITM at baseline, there was approximately a −1.48 diopter more relative myopic refractive progression (p = 0.01). No significant association was found between refractive change and the NITM parameters for either the myopic or emmetropic students after adjusting for the same confounders. However, this relation was significant in the hyperopes (p = 0.01).
ConclusionNITM was only found to be significantly associated with the progression of a myopic refractive shift among the hyperopes.
Myopia is the most common refractive error in the world, especially in the East Asian population.1–4 Our previous studies found that the younger generation was predicted to be approximately 1.94 D and 1.03 D more myopic and have 1.53 mm and 0.57 mm longer axial length than their parental generation (i.e., a generational myopic shift and generational axial length shift) in urban Beijing and in rural Handan, respectively.5–7 The urban and rural generational myopic and axial length shift, and the different magnitudes of these shifts in various regions of China, suggested that environmental factors, such as near work demands, likely play an important role in myopia development in the younger population.5,6
Nearwork-induced transient myopia (NITM) refers to the small and transient myopic shift in the refractive state of the eye at far induced by a period of sustained near work, with near work being one of the most important myopigenic environmental factors currently known.8–12 NITM reflects an inability of the crystalline lens to reduce its power appropriately and rapidly, thus exhibiting an accommodative aftereffect/hysteresis phenomenon of physiological origin, with subsequent far focus.13,14
Initial NITM magnitude and its decay duration are the two key parameters used to describe the accommodative response after a sustained nearwork task.14 The initial NITM magnitude is defined as the dioptric difference between the immediate pre- and immediate post-near task distance refractive state. The decay duration, or decay time, represents the amount of time for this transient accommodative response to return back to the pretask baseline level. These two NITM parameters can be influenced by refractive group.12,14,15 It was reported that they were both increased in myopes as compared to either emmetropes or hyperopes.12,15 Therefore, it has been proposed some years ago that NITM, which produces small and chronic retinal defocus, may be one of many possible environmentally-based, myopigenic, nearwork contributory factors to permanent myopia.16 Another factor which can influence the NITM parameters is the near task duration, with NITM being positively correlated with near task duration.14
The Beijing Myopia Progression Study (BMPS) was a 3-year cohort investigation that commenced July 2010. The main purpose was to determine the possible relation between NITM and permanent myopia. From the baseline data, three response profiles of NITM were found: (1) non-induced, i.e., NITM could not be induced during the 5-minute near task period; (2) complete decay, i.e., NITM could be induced and decayed completely to the pretask level during the 3-minute posttask period (the decay time was 180 s or less); and (3) incomplete decay, i.e., NITM could be induced but decayed incompletely.17 In addition, the initial NITM amount and decay time were larger among the myopic students (0.18 ± 0.16 D, 50 s) than either the emmetropic (0.09 ± 0.13 D, 30 s) or hyperopic (0.10 ± 0.19 D, 20 s) students.17 Furthermore, myopes had the lowest proportion of non-induced NITM when compared to either the emmetropes or hyperopes (10.6% vs. 21.7% and 26.3%, respectively), and the highest proportion of incomplete NITM decay when compared to either the emmetropes or hyperopes (37.9% vs. 19.6% and 29.0%, respectively).17 This suggested that myopic eyes may have more refractive error susceptibility and progression related to near work, per the proposal of Hung & Ciuffreda.16 Per this proposal, the residual NITM would act like the addition of a low-powered plus lens that would reduce the accommodative stimulus, and in turn reduce the accommodative response and correlated accommodative steady-state error. With many repetitions over many months of prolonged nearwork, these repeated changes in the now-reduced far-near defocus magnitude have been proposed to trigger axial elongation, and hence follow the principle of emmetropization for eventual attainment of clear retinal imagery at near, and thus more myopia. However, from the cross-sectional data, it was not clear whether any presumed near work susceptibility accelerated the development of myopia, or it was a result of the myopia per se. Thus, it is important to determine if the refractive error-based susceptibility related to near work was associated with the progression of refractive error. Thus, the purpose of the present study was to report the natural change of NITM and its possible association with the progression of refractive error in Beijing urban school children.
MethodsSubjectsThe study design, procedures, and baseline characteristics of the BMPS were reported in detail elsewhere.17 Briefly, children (aged from 6 to 17 years) from schools in Beijing were recruited from July to September 2010. The inclusion criteria for the current study were: (1) best-corrected visual acuity (BCVA) 0.1 (log minimum angle of resolution, LogMAR) or better; and (2) completed NITM and cycloplegic refraction tests at baseline and at the last follow-up. The exclusion criteria for the current study were: (1) presence of amblyopia and/or strabismus; (2) history of surgery for strabismus, intraocular surgery, or penetrating ocular trauma; (3) use of orthokeratology, atropine, multifocal spectacles, or other treatments that could influence either the measurement of NITM or refraction; and (4) severe medical/ocular health problems. The baseline vision examination of the students included visual acuity, NITM testing, ocular biometry, cycloplegic refraction, and a detailed myopia-related questionnaire. Subsequently, the enrolled students were invited to be reexamined (including ocular biometry, cycloplegic refraction, and the questionnaire) at a similar time in the years of 2011, 2012, and 2013. The NITM testing was performed at baseline and in the years of 2011 and 2012.
The study followed the tenets of the Declaration of Helsinki and was approved by the Beijing Tongren Hospital Ethics Committee. All participants (children and their parents) signed a written informed consent/assent.
NITM testingThe detailed procedure of NITM testing has been described elsewhere.17 Briefly, all students were seated in total darkness for 3 min to allow for the dissipation of potential transient accommodative aftereffects. Then, the distance refractive error of the right eye was obtained objectively using the dynamic model (5 Hz sampling, reported precision of 0.01D) of a binocular, open-field, infrared autorefractor (WAM-5500; Grand Seiko Co., Ltd. Hiroshima, Japan), while the subject binocularly-viewed and focused on 20/30 Snellen letters at 6 m with full distance refractive correction in place. Ten seconds of autorefraction measurements were obtained. Then, the students were asked to identify small differences in pairs of pictures at a distance of 20 cm (5D) placed in front of the autorefractor during the sustained 5-min near task period. Immediately after the 5-min near task, the paired pictures were removed quickly (less than 2 s), and the students were asked to focus immediately on the distant Snellen letters once again. The distance refractive error was then assessed continuously for the post-task period of 3 min. Students were queried about target clarity periodically to ensure that they were focusing accurately.
After the data acquisition, the mean spherical equivalent (MSE, of all measurements for each time bin interval of 10 s) was calculated. The MSE of the posttask minus pretask value represented the NITM dioptric magnitude. Initial NITM was calculated over the first 10-s interval. Decay time was defined the time taken for the NITM magnitude to dissipate precisely to the pretask distance baseline level and be maintained for at least 10 s. The NITM decay area (DA) was defined as the area under the NITM plot, which equaled the NITM magnitude added over time across each data bin interval (i.e., average cumulative decay over time). The initial NITM and its decay area were calculated for each student, and then they were averaged within each refractive group, and also the overall group to obtain the mean data. It should be noted that there was no specified decay time value if NITM was not induced during the 5-min near task. Moreover, the decay time was specified as greater than 180 s if the NITM magnitude did not dissipate precisely to the pretask distance baseline level in the 3-minute-posttask interval. Hence, only the decay profile types (non-induced, complete decay, and incomplete decay) and not the mean value of the decay time were determined.
Refractive errorAll students received a cycloplegic autorefraction (WAM-5500; Grand Seiko Co., Ltd. Hiroshima, Japan) after NITM testing during each visit, whereas the parents received a non-cycloplegic autorefraction (Accuref-K9001, Shin Nippon, Japan) during the baseline examination. Cycloplegic autorefraction was performed 20 min after instilling 3 drops of cyclopentolate 1% (Cyclogyl, Alcon). Three readings were obtained in each eye and averaged within and then across in each group.
Children were divided into three groups based on the spherical equivalent (SE) of their cycloplegic refractive error of the right eye at baseline. Myopes were classified as having a SE < −0.5D; emmetropes were classified as −0.50 ≤ SE ≤ + 0.50D; and hyperopes were classified as SE > + 0.50D.17 Refractive change was defined as the cycloplegic SE at follow up minus the cycloplegic SE at baseline.
Data analysisThe non-normally-distributed parameters (initial NITM, decay area, decay time, and spherical equivalent) were presented as the median (lower quartile, upper quartiles), and they were compared using the Wilcoxon test. Both univariate and multivariate regression (after adjusting for the children's age, gender, baseline cycloplegic refraction, paternal refraction, maternal refraction, near work time, and outdoor time) between the refractive change and NITM parameters was also performed using generalized linear models. Statistical analysis was performed with Statistical Analysis System for Windows version 9.1.3 (SAS Inc., Cary, NC). A p-value less than 0.05 was considered to be statistically significant.
ResultsThere were 386 students enrolled at the baseline of BMPS, and 223 (57.8%) of the students with NITM and cycloplegic refractive data at both baseline and the follow-up examinations were enrolled for this study. The mean follow-up time was 35.6 ± 1.1 months. There were 109 boys (48.9%) and 114 (51.1%) girls. There were 142 myopic (63.7%), 32 emmetropic (14.4%), and 49 hyperopic (22.0%) students according to the baseline cycloplegic refraction. The median (lower quartile, upper quartiles) annual cycloplegic refractive change was −0.45 (−0.73, −0.21) D in these 223 children. Furthermore, the annual refractive change was −0.50 (−0.73, −0.25) D and −0.39 (−0.67, −0.21) D in the boys and girls (p = 0.20), and was −0.45 (−0.75, −0.21) D, −0.54 (−0.86, −0.23) D, and −0.35 (−0.63, −0.26) D in the myopes, emmetropes, and hyperopes (p = 0.38), respectively.
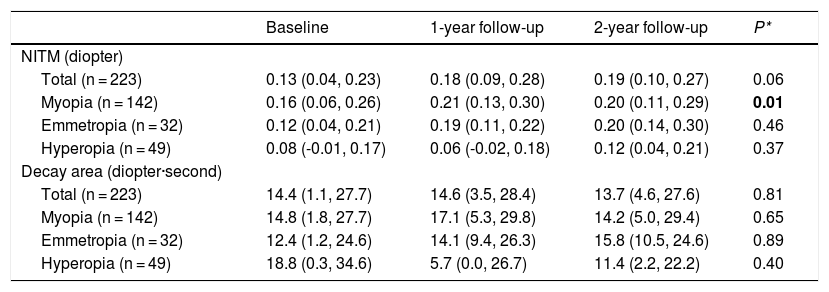
Natural change of NITMAs introduced above and as stated earlier, only the overall distribution of the decay time was presented. The initial NITM magnitude and its decay area are presented in Table 1. The initial NITM magnitude (median, lower and upper quartiles) increased significantly in the overall myopic students from 0.16 (0.06, 0.26) D at baseline to 0.21 (0.13, 0.30) D and 0.20 (0.11, 0.29) D at the one-year and two-year follow-up, respectively (p = 0.01), but not significantly changed for either the overall emmetropic or hyperopic students. The decay area was not significantly changed in the overall, myopic, emmetropic, or hyperopic students (Table 1).
Initial NITM and its decay area at each test time.
| Baseline | 1-year follow-up | 2-year follow-up | P* | |
|---|---|---|---|---|
| NITM (diopter) | ||||
| Total (n = 223) | 0.13 (0.04, 0.23) | 0.18 (0.09, 0.28) | 0.19 (0.10, 0.27) | 0.06 |
| Myopia (n = 142) | 0.16 (0.06, 0.26) | 0.21 (0.13, 0.30) | 0.20 (0.11, 0.29) | 0.01 |
| Emmetropia (n = 32) | 0.12 (0.04, 0.21) | 0.19 (0.11, 0.22) | 0.20 (0.14, 0.30) | 0.46 |
| Hyperopia (n = 49) | 0.08 (-0.01, 0.17) | 0.06 (-0.02, 0.18) | 0.12 (0.04, 0.21) | 0.37 |
| Decay area (diopter·second) | ||||
| Total (n = 223) | 14.4 (1.1, 27.7) | 14.6 (3.5, 28.4) | 13.7 (4.6, 27.6) | 0.81 |
| Myopia (n = 142) | 14.8 (1.8, 27.7) | 17.1 (5.3, 29.8) | 14.2 (5.0, 29.4) | 0.65 |
| Emmetropia (n = 32) | 12.4 (1.2, 24.6) | 14.1 (9.4, 26.3) | 15.8 (10.5, 24.6) | 0.89 |
| Hyperopia (n = 49) | 18.8 (0.3, 34.6) | 5.7 (0.0, 26.7) | 11.4 (2.2, 22.2) | 0.40 |
NITM: nearwork-induced transient myopia.
Presented as median (lower quartiles, upper quartiles).
P*: tested by repeated analysis of variance performed by generalized linear model.
Significant value in bold.
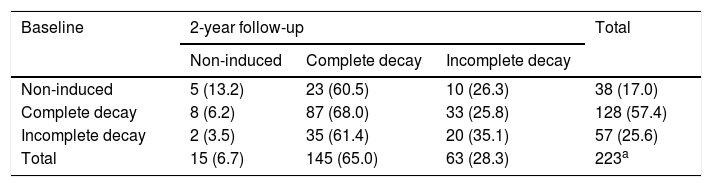
The NITM decay types are presented in Table 2. The overall proportion of NITM decay type shifted significantly from the non-induced type at baseline (non-induced: 17.0%, complete decay 57.4%m nbb, incomplete decay 25.6%) to the incomplete decay type at the 2-year follow-up (non-induced: 6.7%, complete decay 65.0%, incomplete decay 28.3%, McNemar's test, p = 0.01).
Number (proportion) of different NITM decay profile types at baseline and at the 2-year follow-up in the overall students.
| Baseline | 2-year follow-up | Total | ||
|---|---|---|---|---|
| Non-induced | Complete decay | Incomplete decay | ||
| Non-induced | 5 (13.2) | 23 (60.5) | 10 (26.3) | 38 (17.0) |
| Complete decay | 8 (6.2) | 87 (68.0) | 33 (25.8) | 128 (57.4) |
| Incomplete decay | 2 (3.5) | 35 (61.4) | 20 (35.1) | 57 (25.6) |
| Total | 15 (6.7) | 145 (65.0) | 63 (28.3) | 223a |
NITM: nearwork-induced transient myopia.
The univariate regression analysis between the children’s annual refractive change and the baseline NITM parameters (initial NITM magnitude, decay area, and decay type) revealed that only the initial NITM magnitude was negatively associated with the refractive change (β = −0.39, p = 0.03), which was only found in the hyperopic students, i.e., the larger the initial NITM magnitude at baseline, the more relative myopic refractive change in the hyperopic students. This remained a significant association after adjusting for the children’s age, gender, and baseline cycloplegic refraction (β = −0.41, p = 0.03). When further adjusted for paternal refraction, maternal refraction, near work time, and outdoor time, the initial NITM magnitude was still negatively associated with refractive change in the hyperopic students (β = −0.51, p = 0.01). However, no significant association was found between refractive change and the other NITM parameters for the hyperopic students. Additionally, there were no significant associations found between the refractive change and the NITM parameters for either the myopic or emmetropic students (Table 3).
Multivariate regression analysisa of the associations between annual refractive change (diopter) and baseline NITM parameters in students in Beijing.
| Myopia | Emmetropia | Hyperopia | Total | |
|---|---|---|---|---|
| Initial NITM (diopter) | −0.14 (0.31) | 0.06 (0.75) | −0.51 (0.01) | −0.17 (0.07) |
| Decay area (diopter·second) | −0.001 (0.30) | 0.001 (0.44) | −0.001 (0.55) | 0.000 (0.86) |
| Decay type | −0.04 (0.31) | 0.04 (0.72) | 0.01 (0.83) | −0.03 (0.38) |
NITM: nearwork-induced transient myopia.
Significant value in bold.
In the baseline study of the BMPS, a significant difference among refractive groups was found for both the initial NITM magnitude and its decay time, i.e., a greater initial NITM magnitude and a longer NITM decay time was found in the myopes when compared to either the emmetropes or hyperopes,17 We also found a correlation between the initial NITM magnitude and the cycloplegic refractive error for the overall students (r = −0.24, p < 0.001), and a similar trend for correlation in the hyperopes (r = 0.22, p = 0.058).17 Furthermore, refractive error susceptibility was found. Myopic children had the highest proportion of induced NITM during the 5-minute near task, and the highest proportion of incomplete NITM decay to pretask levels during the 3-minute posttask period, when compared to either the emmetropic or hyperopic children.17
Two previous studies have also assessed the characteristics of NITM in children.12,18 Wolffsohn reported that Hong Kong Chinese juvenile myopes had greater initial NITM than found in their emmetropes (0.47 ± 0.46 D vs. 0.19 ± 0.58 D, respectively, p < 0.001), and furthermore lacked significant decay of NITM after either a 5.0 or 2.5D near task demand (p = 0.30).12 These results suggested that preadolescent, myopic Hong Kong Chinese children were more highly susceptible than their emmetropic peers to blur-driven, NITM induced by sustained near vision. This was consistent with earlier pilot findings, in which 30% of young Caucasian children (ages 4–7 years) maintained elevated and non-decayed NITM over a 3-minute post-task period following a 5-minute period of sustained near work (5D with a continuous cognitive task demand).18 These studies suggest a distinguishing feature of NITM, namely its persistence, and furthermore the apparent lack of dependence on the level of near accommodative demand, in some young children.19
Atropine eye drops with different concentrations have been reported to slow down the myopic progression in myopes.20–22 Recently, a randomized study assessed the efficacy of a low-concentration of atropine (0.01%) on the initial NITM magnitude among Chinese myopic children aged 6–15 years.23 They reported that the initial NITM magnitude was significantly reduced for approximately 0.45D after 7 and 14 days of instilling atropine.23 This study suggests, to some extent, that atropine may slow down the myopia progression through reducing initial NITM magnitude. However, there was no direct data on the association between NITM and refractive change, so this remains speculative.
To our knowledge, this is the first study that investigated longitudinal, natural changes of NITM, and its possible association with the progression of refractive error in children. There were several new and important findings. First, the initial NITM magnitude increased slightly over the years in the myopic students. However, the magnitude increase was too small to reach clinical significance in terms of reducing distance visual clarity. Second, the overall proportion of non-induced NITM at baseline decreased when compared to that found at the 2-year follow-up period (17.0% to 6.7%). This suggests that the children’s susceptibility, or accommodative aftereffects, to sustained near-work increased over the test years. Lastly, and most importantly, among the hyperopic children, smaller initial NITM magnitude was found to be significantly associated with less myopic refractive change. However, no significant association was found among either the myopic or emmetropic children, although refractive error susceptibility was greater among myopic eyes, at baseline. Ciuffreda et al. reported that hyperopic young adults manifested a paradoxical hyperopic refractive shift after a sustained period of near work.15,24 The reason for the difference between Ciuffreda et als and the current finding may due to different ages (adults vs. students less than 18 years old), ethnicity, daily activities, and sample size previous studies (16 and 44 vs. 223 in the current study).
In the present study, although the hyperopic children exhibited a relatively small initial NITM (i.e, transient myopic shift), they potentially exerted more ciliary muscle-based accommodation, since the majority of them did not wear a refractive correction (81.6% at baseline and 68.6% at the 3-year follow-up). The hyperopic children presented with a more variable NITM response profile after a period of sustained near work (i.e., increased and variable NITM magnitude at the middle and later post-task period) at both the baseline and at the two-year follow-up. In addition, approximately 30% of the hyperopes also exhibited incomplete decay of NITM. Moreover, and as reported in previous work on the same study sample, we found that the hyperopic students exhibited a significantly greater difference between their cycloplegic and non-cycloplegic refraction at both baseline and at follow-up, as compared to the myopic and emmetropic students.25 In general, the above evidence suggested a greater ciliary spasm/accommodative aftereffect among the hyperopic children in their daily life, as might be expected. Hence, more spasm of the ciliary muscle, and related variability of the NITM decay response, may be the reason that the hyperopic children manifested more myopic refractive change. This warrants further investigation.
There were some potential limitations in the present study. First, the sample size was relatively small, and the follow-up was relatively short. This may result in lack of a significant association between the inherent small values of NITM and relatively small refractive change in the myopic and emmetropic students. Second, the proportion of refractive error types at baseline was somewhat uneven due to the hospital-based design of this study, thus resulting in more myopic children than either emmetropic and hyperopic ones being enrolled at baseline (for example, the proportion of myopic of 15-year-old girls: 66.8% in the current study5 vs. 55.0% in a suburb of Beijing1). This may also be the reason for lack of a significant increase of NITM magnitude in the emmetropic students.
In summary, our primary new finding was that only among the hyperopic children was NITM associated with the progression of a relative myopic refractive shift, possibly through a mild spasm of the ciliary muscle and increased variability of NITM decay response. Interestingly, no such association was found for either the myopic or emmetropic cohorts.
Financial supportThe study was supported by the Beijing Science & Technology Novel Star Program (2009B44).
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors thank Dr. Yi Cao Zhang (Anyang Eye Hospital), Dr. Xiao Dong Yang (Nanjing Tongren Hospital), Dr. Qian Jia (Handan Eye Hospital), Dr. Yue Wu (Beijing Xuanwu Hospital, Capital Medical University), and Dr. Xiao Gu Cai (Beijing Tongren Hospital, Capital Medical University) for their invaluable assistance in data collection.





