

Claims that coloured filters aid reading date back 200 years and remain controversial. Some claims, for example, that more than 10% of the general population and 50% of people with dyslexia would benefit from coloured filters lack sound evidence and face validity. Publications with such claims typically cite research using methods that have not been described in the scientific literature and lack a sound aetiological framework.
Notwithstanding these criticisms, some researchers have used more rigorous selection criteria and methods of prescribing coloured filters that were developed at a UK Medical Research Council unit and which have been fully described in the scientific literature. We review this research and disconfirm many of the more extreme claims surrounding this topic. This literature indicates that a minority subset of dyslexics (circa 20%) may have a condition described as visual stress which most likely results from a hyperexcitability of the visual cortex. Visual stress is characterised by symptoms of visual perceptual distortions, headaches, and eyestrain when viewing repetitive patterns, including lines of text. This review indicates that visual stress is distinct from, although sometimes co-occurs with, dyslexia. Individually prescribed coloured filters have been shown to improve reading performance in people with visual stress, but are unlikely to influence the phonological and memory deficits associated with dyslexia and therefore are not a treatment for dyslexia.
This review concludes that larger and rigorous randomised controlled trials of interventions for visual stress are required. Improvements in the diagnosis of the condition are also a priority.
Las aseveraciones acerca de que los filtros coloreados ayudan a la lectura se remontan 200 años atrás, y siguen siendo controvertidas. Por ejemplo, algunas afirmaciones relativas a que el 10% de la población general y el 50% de las personas disléxicas podrían beneficiarse de los filtros coloreados carecen de evidencia y de validez firmes. Las publicaciones que incluyen dichas afirmaciones citan, normalmente, investigaciones que hacen uso de métodos no descritos en la literatura científica y que carecen de marcos etiológicos sólidos.
A pesar de estas críticas, algunos investigadores han utilizado unos criterios y métodos de selección más rigurosos para la prescripción de filtros coloreados, desarrollados en una unidad del Medical Research Council del Reino Unido y que se han descrito cuidadosamente en la literatura científica. Revisamos todas estas investigaciones que desmienten muchas de las aseveraciones más extremas que rodean a esta cuestión. Esta literatura científica consistente indica que un subgrupo minoritario de disléxicos (de alrededor del 20%) puede padecer una afección médica descrita como estrés visual, que deriva muy probablemente de la hiperexcitabilidad de la corteza visual. El estrés visual se caracteriza por síntomas de distorsión de la percepción visual, cefaleas, y fatiga visual al visualizar patrones repetitivos, incluyendo las líneas de texto. Esta revisión indica que el estrés visual es diferente a la dislexia, aunque a veces coexisten ambas situaciones. Se ha demostrado que los filtros coloreados individualmente prescritos mejoran el desempeño lector en personas con estrés visual, pero es improbable que mejoren los déficits fonológicos y de memoria que se asocian a la dislexia, por lo que no constituyen un tratamiento para la misma.
Esta revisión concluye que se precisan más ensayos controlados y aleatorizados sobre intervenciones para el estrés visual. También son prioritarias las mejoras diagnósticas de dicha afección.
Claims that coloured filters ease eyestrain when reading originate from the 1780s,1 and in 1964 Critchley described a dyslexic child who could only read on coloured paper.2 Meares described a cluster of symptoms3 of perceptual distortion when reading and Irlen claimed the distortions were common and were reduced by her individually prescribed coloured filters4; claims that remain controversial.5,6 Previous reviews of this condition, often now called visual stress (VS), have reached discrepant conclusions.5,7 VS is characterised by symptoms of asthenopia and visual perceptual distortions when observing striped patterns, including lines of text.8 This field lacks large randomised controlled trials of the type that would be required for the validation of new drugs. This situation is somewhat analogous to that faced recently by authors reviewing treatments for intermittent exotropia9: a recent Cochrane review (on intermittent exotropia) was unhelpful because it had only found one appropriate study. These authors dealt with this dilemma in a pragmatic way, by carrying out a review of the best available evidence.9 The present authors have adopted a similar pragmatic approach to review the best available evidence for treatments of visual stress.
The initial approach for the treatment of visual stress, developed by Irlen, has been criticised because the system has not been fully described in the scientific literature,10 does not systematically sample colour space,11,12 and is not typically administered by eyecare professionals. A newer system using “Intuitive overlays” (IO), the “Intuitive colorimeter” (IC), and Cerium Precision Tinted Lenses was developed by Wilkins at the UK Medical Research Council (MRC) Applied Psychology Unit. This system is fully described in the scientific literature,11,13,14 systematically and efficiently samples colour space,11,13 and has been shown to have the properties required for an appropriate method.14–17 This system is used by eyecare professionals which is important clinically to ensure that symptoms due to ophthalmic conditions are alleviated before colour is used.18,19 For these reasons, this paper reviews evidence from research using the Wilkins (MRC) system.
The condition that is purportedly helped by coloured filters has been given various names,20 most recently visual stress21 or pattern related visual stress (PRVS).22 Visual stress has other meanings,23–25 but as noted below in the discussion most studies in this field to date are likely to have included a heterogeneous sample. PRVS relates the condition to the likely aetiology26 and PRVS may be the most appropriate term for studies that include a pattern glare test, although at present this is only a minority of studies. For the present review the widely used term visual stress will be used. intuitive overlays11 are sheets of coloured plastic placed on the page and in this review Precision Tinted Lenses describes coloured lenses prescribed with the IC.13 The term coloured filters is used generically to describe intuitive overlays and Precision Tinted Lenses prescribed with the IC.
The prevalent view on the aetiology of VS is that the striped patterns caused by text27 over-stimulate a hyper-excitable visual cortex.28 It is hypothesised that by altering the spectral composition of the retinal image with coloured filters, cortical activity29 can be rearranged so as to avoid strong local excitation in hyperexcitable orientation columns of the visual cortex.30 Research continues investigating this hypothesis and the nature of visual discomfort has been31–40 the topic of a recent review.26
Reading difficulties, dyslexia, and VSA comprehensive review (the Rose report) defined dyslexia as a learning difficulty that primarily affects the skills involved in accurate and fluent word reading and spelling with characteristic features of difficulties in phonological awareness, verbal memory and verbal processing speed.41 These non-visual factors are likely to be causes of the poor reading. The report acknowledges that sensory or motor co-ordination difficulties can occur alongside dyslexia and includes VS among these conditions, but stresses that there is no evidence of a causal link between VS and dyslexia. This is also the conclusion of the present review: VS may contribute to the overall difficulties that a dyslexic child experiences in the classroom but is unlikely to be a cause of dyslexia. It is therefore not appropriate for eyecare practitioners or others dispensing coloured filters to claim that they can treat dyslexia.
The Rose report indicates that VS co-occurs with dyslexia and the two studies that investigate this hypothesis find a higher prevalence of VS in dyslexia than in good readers.42,43 In both studies, the statistical significance was marginal. A third concordant study (also lacking statistical power) indicates that VS is more likely to be problematic when it co-occurs with dyslexia.44 It is clear from the literature that most people with dyslexia do not have VS (see next section) and therefore studies investigating the effect of coloured filters on samples selected as having dyslexia45 suffer from selection bias and will be underpowered. It is perhaps surprising that not all studies of VS have studied people with VS45,46 and reviews that fail to make the differentiation between dyslexia and VS are likely to reach invalid conclusions.
Diagnosis of VSVS is suspected when people report symptoms of visual perceptual distortions, eyestrain, or headaches during reading. Four approaches have been used to detect VS:
- 1.
Questionnaire-based rating scales.39,44,47
- 2.
Pattern glare test (PGT),22,48–50
- 3.
Sustained voluntary use of IO.12,51,52
- 4.
Improvement in reading (typically, with Wilkins Rate of Reading Test; WRRT)53,54 or task performance22,43 with IO.
An additional criterion is to exclude patients with an ophthalmic problem that may account for their symptoms. Although important for clinical practice, this approach is not always adopted in research studies but is unlikely to be a significant confounder because ophthalmic factors are infrequent correlates of VS.8,55–57
Early research confirmed anecdotal observations that the symptoms of visual stress worsen with prolonged reading and a significant effect at reading normal text is only to be expected after about 10min.53 This could make clinical testing impractical and Wilkins therefore developed the WRRT which uses small crowded text to induce the symptoms of VS sooner and which can demonstrate an effect of colour in a simple four minute test.54
VS seems to lie on a spectrum from mild to highly symptomatic. Large studies investigating the effect of IO with the WRRT show that about one third of those choosing overlays read >5% faster with the overlay whilst 5% of unselected schoolchildren read >25% faster.58 Indeed, the spectrum of VS can be characterised, from a performance perspective, as the percentage improvement in WRRT performance with overlays. A low criterion (e.g., >5% improvement at WRRT) is likely to identify everyone with VS but also many without clinically significant VS (high sensitivity but low specificity). A high criterion (e.g., >50% improvement) is likely to miss a significant number of people with symptomatic VS but detect very few who do not have VS (high specificity and low sensitivity). An early tendency to use >5% as a WRRT cut-off will over-diagnose VS42 and a recent analysis indicates that >15% is likely to be the most appropriate criterion, at least for children.59 A re-analysis of previously reported data on prevalence42 using this criterion suggests VS occurs in about 20% of children with dyslexia. This indicates that Irlen's approach, which can detect VS in close to 80% of people with reading difficulties,60 over-diagnoses the condition.
The use of IO in diagnosing visual stress has been criticised,7 because of the use of “the intervention under evaluation to screen and enrol subjects”. The use of a treatment for diagnosis also occurs for other conditons61–63 and indeed many conditions are diagnosed purely on the presence of symptoms and exclusion of other causes.64 Nonetheless, the present authors agree that improvements need to be made in the diagnosis of VS (see discussion).
This review seeks to address the following research question: “Do individually prescribed coloured filters alleviate symptoms attributed to VS when reading, and improve visual performance?” The selection criteria for the review can be summarised as studies of people diagnosed with VS and using IO or the IC. These criteria are specified in more detail in the next section.
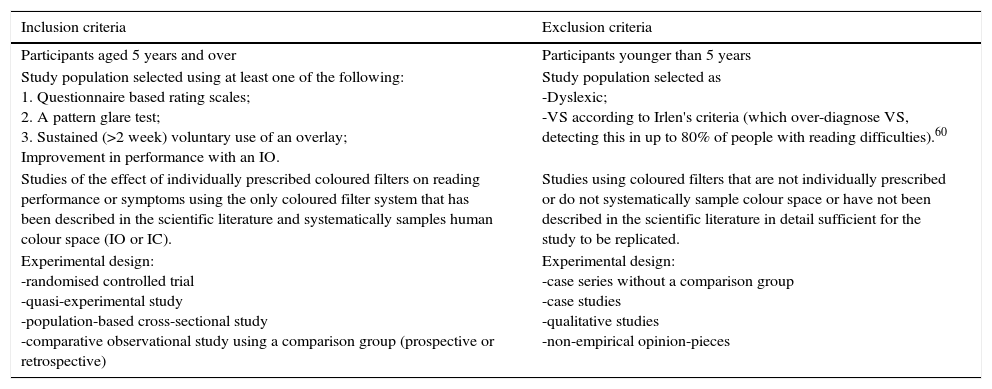
MethodsEligibilityThe eligibility criteria for this review are shown in Table 1.
Summary of review eligibility criteria.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Participants aged 5 years and over | Participants younger than 5 years |
| Study population selected using at least one of the following: 1. Questionnaire based rating scales; 2. A pattern glare test; 3. Sustained (>2 week) voluntary use of an overlay; Improvement in performance with an IO. | Study population selected as -Dyslexic; -VS according to Irlen's criteria (which over-diagnose VS, detecting this in up to 80% of people with reading difficulties).60 |
| Studies of the effect of individually prescribed coloured filters on reading performance or symptoms using the only coloured filter system that has been described in the scientific literature and systematically samples human colour space (IO or IC). | Studies using coloured filters that are not individually prescribed or do not systematically sample colour space or have not been described in the scientific literature in detail sufficient for the study to be replicated. |
| Experimental design: -randomised controlled trial -quasi-experimental study -population-based cross-sectional study -comparative observational study using a comparison group (prospective or retrospective) | Experimental design: -case series without a comparison group -case studies -qualitative studies -non-empirical opinion-pieces |
We conducted systematic searches using the following databases: PubMed, ERIC, Cochrane Central Register of Controlled Trials, PubPsych (see Supplementary material). We supplemented these searches by examining databases of publications held by the authors and other researchers in the field, and by hand-searching the bibliographies of included studies.
We conducted systematic searches using the following databases: PubMed, ERIC, Cochrane Central Register of Controlled Trials, PubPsych (see Supplementary material). We supplemented these searches by examining databases of publications held by the authors and other researchers in the field, and by hand-searching the bibliographies of included studies.
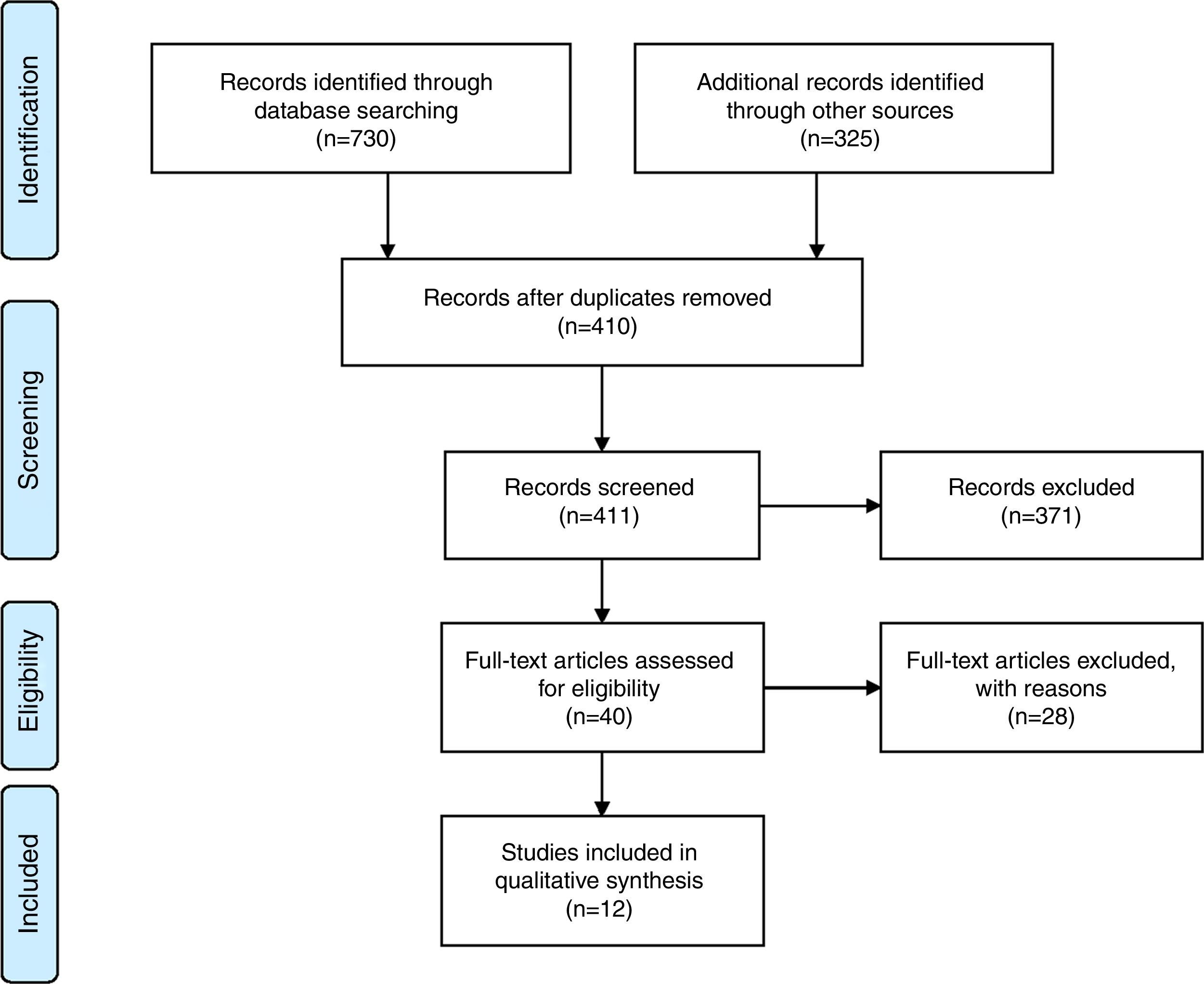
Selection, data extraction, appraisal, and synthesisA PRISMA flow Chart summarising the review process is in Fig. 1.

One reviewer screened citation information to remove duplicates. Abstracts were screened and irrelevant manuscripts removed. For the remaining manuscripts, the full papers were studied and reviewed by both authors to determine those that should be included. Sections of the review referring to research by one of the review authors was written by a different review author not involved in that work. CASP criteria were used to assess bias.65 The principal summary measure is difference in means.
ResultsThe results of the literature review are summarised in three sections, two relating to research with IO and one to research with the IC.
In the first section, controlled trials using IO are reviewed. Controlled trials have limitations and an over-reliance on controlled trials has been criticised.66,67 Indeed Hill, the architect of the randomised controlled trial (RCT), commented that “any belief that the controlled trial is the only way would mean not that the pendulum had swung too far but that it had come right off the hook”.68 The second section reviews complementary approaches.
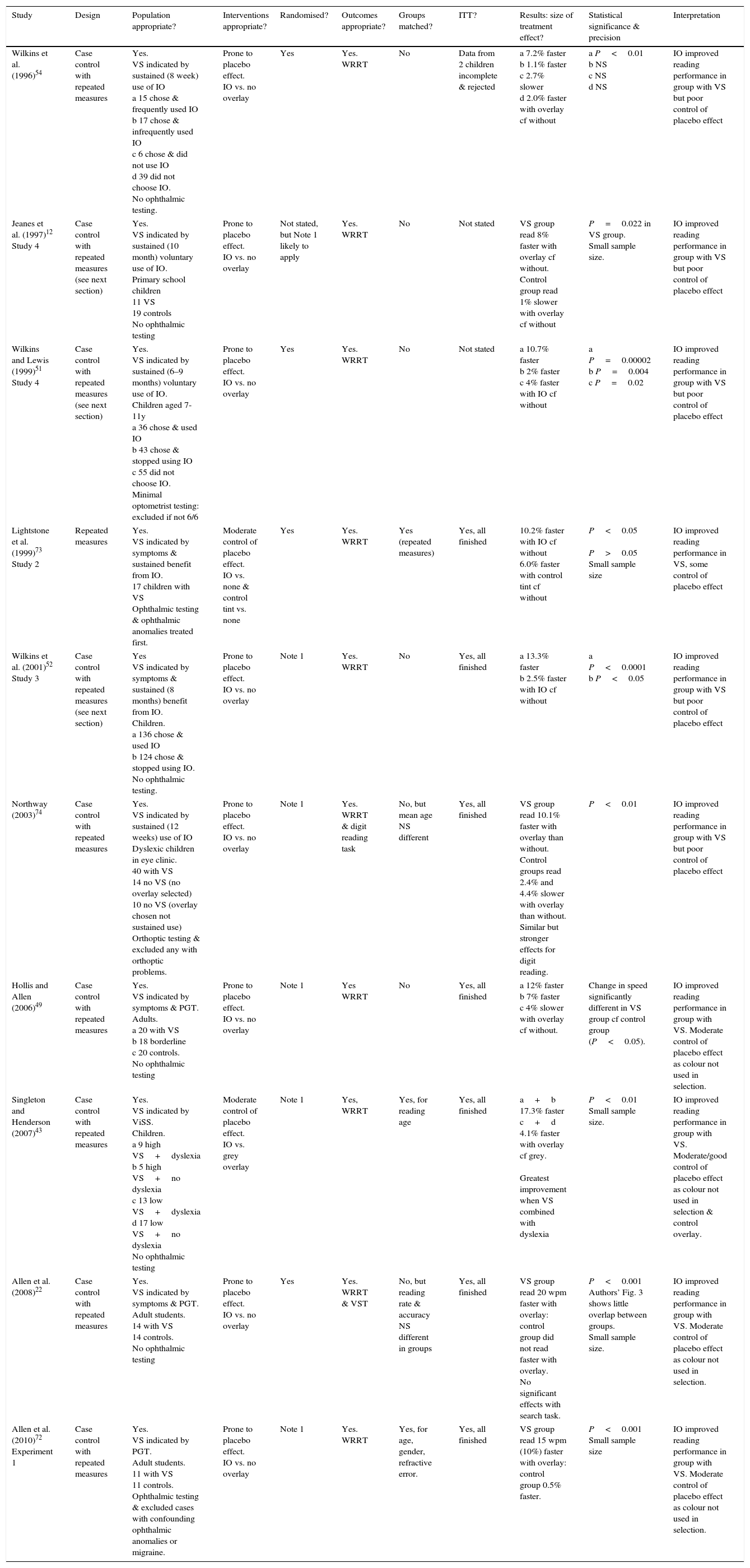
Controlled trials using intuitive overlaysTable 2 evaluates, using CASP criteria,65 studies of the effect of IO on reading, or related performance, in populations selected as having VS. Controlled trials with IO which applied at least one of the four diagnostic criteria for VS detailed in the introduction and methods sections and which used a different method to assess the effect of IO use are included.
Summary of controlled trials of intuitive overlays (IO) in populations selected as having VS. Key CASP65 critical appraisal criteria for assessing bias are detailed in the columns, with the exception of two CASP criteria: masking (it is not possible to double mask overlay studies) and it is assumed that groups were treated equally as all studies are repeated measures trials. Abbreviations: EE, eye examination; ITT, intention to treat (were all of the participants who entered the trial properly accounted for at its conclusion?); NS, not significant; PGT, pattern glare test; VDS, Visual Discomfort Scale; ViSS, computerised visual stress screener; VST, visual search task; WPM, words per minute; WRRT, Wilkins Rate of Reading Test. P-values are two-tailed. Note 1: in these studies the WRRT was carried out as recommended in the test instructions using an ABBA order to control for practice effects.52
| Study | Design | Population appropriate? | Interventions appropriate? | Randomised? | Outcomes appropriate? | Groups matched? | ITT? | Results: size of treatment effect? | Statistical significance & precision | Interpretation |
|---|---|---|---|---|---|---|---|---|---|---|
| Wilkins et al. (1996)54 | Case control with repeated measures | Yes. VS indicated by sustained (8 week) use of IO a 15 chose & frequently used IO b 17 chose & infrequently used IO c 6 chose & did not use IO d 39 did not choose IO. No ophthalmic testing. | Prone to placebo effect. IO vs. no overlay | Yes | Yes. WRRT | No | Data from 2 children incomplete & rejected | a 7.2% faster b 1.1% faster c 2.7% slower d 2.0% faster with overlay cf without | a P<0.01 b NS c NS d NS | IO improved reading performance in group with VS but poor control of placebo effect |
| Jeanes et al. (1997)12 Study 4 | Case control with repeated measures (see next section) | Yes. VS indicated by sustained (10 month) voluntary use of IO. Primary school children 11 VS 19 controls No ophthalmic testing | Prone to placebo effect. IO vs. no overlay | Not stated, but Note 1 likely to apply | Yes. WRRT | No | Not stated | VS group read 8% faster with overlay cf without. Control group read 1% slower with overlay cf without | P=0.022 in VS group. Small sample size. | IO improved reading performance in group with VS but poor control of placebo effect |
| Wilkins and Lewis (1999)51 Study 4 | Case control with repeated measures (see next section) | Yes. VS indicated by sustained (6–9 months) voluntary use of IO. Children aged 7-11y a 36 chose & used IO b 43 chose & stopped using IO c 55 did not choose IO. Minimal optometrist testing: excluded if not 6/6 | Prone to placebo effect. IO vs. no overlay | Yes | Yes. WRRT | No | Not stated | a 10.7% faster b 2% faster c 4% faster with IO cf without | a P=0.00002 b P=0.004 c P=0.02 | IO improved reading performance in group with VS but poor control of placebo effect |
| Lightstone et al. (1999)73 Study 2 | Repeated measures | Yes. VS indicated by symptoms & sustained benefit from IO. 17 children with VS Ophthalmic testing & ophthalmic anomalies treated first. | Moderate control of placebo effect. IO vs. none & control tint vs. none | Yes | Yes. WRRT | Yes (repeated measures) | Yes, all finished | 10.2% faster with IO cf without 6.0% faster with control tint cf without | P<0.05 P>0.05 Small sample size | IO improved reading performance in VS, some control of placebo effect |
| Wilkins et al. (2001)52 Study 3 | Case control with repeated measures (see next section) | Yes VS indicated by symptoms & sustained (8 months) benefit from IO. Children. a 136 chose & used IO b 124 chose & stopped using IO. No ophthalmic testing. | Prone to placebo effect. IO vs. no overlay | Note 1 | Yes. WRRT | No | Yes, all finished | a 13.3% faster b 2.5% faster with IO cf without | a P<0.0001 b P<0.05 | IO improved reading performance in group with VS but poor control of placebo effect |
| Northway (2003)74 | Case control with repeated measures | Yes. VS indicated by sustained (12 weeks) use of IO Dyslexic children in eye clinic. 40 with VS 14 no VS (no overlay selected) 10 no VS (overlay chosen not sustained use) Orthoptic testing & excluded any with orthoptic problems. | Prone to placebo effect. IO vs. no overlay | Note 1 | Yes. WRRT & digit reading task | No, but mean age NS different | Yes, all finished | VS group read 10.1% faster with overlay than without. Control groups read 2.4% and 4.4% slower with overlay than without. Similar but stronger effects for digit reading. | P<0.01 | IO improved reading performance in group with VS but poor control of placebo effect |
| Hollis and Allen (2006)49 | Case control with repeated measures | Yes. VS indicated by symptoms & PGT. Adults. a 20 with VS b 18 borderline c 20 controls. No ophthalmic testing | Prone to placebo effect. IO vs. no overlay | Note 1 | Yes WRRT | No | Yes, all finished | a 12% faster b 7% faster c 4% slower with overlay cf without. | Change in speed significantly different in VS group cf control group (P<0.05). | IO improved reading performance in group with VS. Moderate control of placebo effect as colour not used in selection. |
| Singleton and Henderson (2007)43 | Case control with repeated measures | Yes. VS indicated by ViSS. Children. a 9 high VS+dyslexia b 5 high VS+no dyslexia c 13 low VS+dyslexia d 17 low VS+no dyslexia No ophthalmic testing | Moderate control of placebo effect. IO vs. grey overlay | Note 1 | Yes, WRRT | Yes, for reading age | Yes, all finished | a+b 17.3% faster c+d 4.1% faster with overlay cf grey. Greatest improvement when VS combined with dyslexia | P<0.01 Small sample size. | IO improved reading performance in group with VS. Moderate/good control of placebo effect as colour not used in selection & control overlay. |
| Allen et al. (2008)22 | Case control with repeated measures | Yes. VS indicated by symptoms & PGT. Adult students. 14 with VS 14 controls. No ophthalmic testing | Prone to placebo effect. IO vs. no overlay | Yes | Yes. WRRT & VST | No, but reading rate & accuracy NS different in groups | Yes, all finished | VS group read 20 wpm faster with overlay: control group did not read faster with overlay. No significant effects with search task. | P<0.001 Authors’ Fig. 3 shows little overlap between groups. Small sample size. | IO improved reading performance in group with VS. Moderate control of placebo effect as colour not used in selection. |
| Allen et al. (2010)72 Experiment 1 | Case control with repeated measures | Yes. VS indicated by PGT. Adult students. 11 with VS 11 controls. Ophthalmic testing & excluded cases with confounding ophthalmic anomalies or migraine. | Prone to placebo effect. IO vs. no overlay | Note 1 | Yes. WRRT | Yes, for age, gender, refractive error. | Yes, all finished | VS group read 15 wpm (10%) faster with overlay: control group 0.5% faster. | P<0.001 Small sample size | IO improved reading performance in group with VS. Moderate control of placebo effect as colour not used in selection. |
Studies that investigated samples whose sole indicator for VS is reporting an immediate improvement in perception with an overlay are not included because this will over-diagnose VS, selecting about 50% of the population.12,51,52,57 The exclusion of these studies (all of which found improved performance with IO)12,51,52,69–71 means that several studies often cited as supporting the use of IO are not included in Table 2. Three of the papers cited in Table 2 included studies that were not designed to be clinical trials but rather to assess prevalence of VS.12,51,52 These papers each contained several studies which together provide a more holistic investigation of VS and are detailed in the next section; only the experiments that constitute controlled trials are described in Table 2.
It is not possible to mask participants in a trial comparing coloured overlays with a control (e.g., grey), and this represents a risk of bias across studies. Nonetheless, all 10 studies in Table 2 found statistically significant improvements in performance with individually selected IO. Some of the studies used testing with colour in their participant selection process (see above). However, it is notable that the four studies that selected participants in other ways (avoiding testing with colour) also found statistically significant benefits from coloured filters.22,43,49,72
Systematic research using intuitive overlaysThere are limitations to research with coloured overlays. Typically, participants are asked a series of questions about symptoms when viewing text. Asking these questions may increase the reporting of symptoms as a result of suggestion, although in the research described below the questions were worded so that there were alternatives to minimise the risk of suggestion. The next stage is to ask participants if coloured overlays reduce their symptoms. Coloured filters will alter the appearance of the page and this may be interpreted by some children as reducing symptoms. This could lead to immediate reports of a reduction in symptoms that, via a placebo effect, leads to improved performance. Since participants will be aware of the colour they have chosen, then they will be aware that a control colour is different and this limits the ability to control for the placebo effect. Various approaches have been used in attempts to minimise these limitations. In particular, three papers12,51,52 have been published which each include several studies investigating different aspects of the effects of IO and which, in each paper, combine to address many of the limitations of overlay studies. The studies within these papers that constitute controlled trials are described above, but these experiments taken out of the context of the other studies in the papers present an incomplete picture. These three papers will now be summarised.
Jeanes et al. (1997)12In Study 1, 152 children aged 5–12 years from two centres were administered a symptom questionnaire and IO test, with 51–54% choosing an overlay. Three months later (Study 2) 75–89% of those given an overlay were still using the overlay and colour choice was retested and found to be reliable. In Study 3, the researchers returned 10 months after the initial testing and 21% of those initially requesting an overlay were still using this.
In Study 4, the 14 children who persisted in using an IO were found to read significantly more quickly with the overlay than without. In contrast, those who did not persist with the overlay read at an almost identical mean speed with and without the overlay. The authors noted that the children who read more rapidly with their overlay might have done so because they became familiar with the use of the overlay. They investigated this in Study 5 by testing a completely new sample of 77 children to see whether performance at the WRRT was predictive of those who would still be using a coloured overlay one school term later. Twenty percent of those tested persisted in the use of an overlay. Those who persisted in using an overlay had read significantly more quickly with the overlay than without when tested at the start of the school term. In contrast, those who did not persist with an overlay had not read significantly more quickly with the overlay than without.
It is possible that the benefit from IO is attributable to reduced contrast. Study 6 investigated this using a grey overlay and showed that grey does not produce the benefit demonstrated with individually selected colour. Participants read fastest with their preferred colour (74.1) and this was significantly faster than with the clear (65.8) and grey (66.3) overlays, but not significantly faster than with a complementary colour (69.7), possibly owing to the modest sample size. Study 7 investigated a new method of group testing with coloured paper, but this was not effective. This may be because only 6 colours were used and later research indicates that this is unlikely to be enough.17,71
In summary, these 7 studies indicate that contrast reduction is not the mechanism for the benefit from IO and demonstrate that it is the children who read significantly faster with an IO who are likely to continue to use it.
Wilkins and Lewis (1999)51In Study 1, the authors attempted to control for the placebo effect by comparing WRRT performance with a chosen overlay with a grey overlay that was labelled “prototype” and given a cover story to generate a placebo effect. The children read significantly more quickly with their chosen overlay than with the placebo. In Studies 2–3, the authors showed that the preferred overlay was associated with improved performance at a new test of “texture segregation”, when of suitable design (Study 3), as well as improvement in WRRT thereby suggesting that some of the improvement in reading speed is perceptual in origin.
Studies 1–3 were limited by evaluating small samples (22–34) of children who were referred to a sensory support service. Study 4 evaluated 133 children who were unselected other than having normal visual acuity. Twenty-seven percent of the sample chose and persisted in using an overlay. Improvement at the WRRT and the texture segregation task with the overlay after several months was significant only for the sustained users.
This study replicates the earlier12 finding that the children who demonstrate sustained use of an overlay are those that also exhibit a significant improvement in performance with the overlay both before and after experience of its use. The findings of Study 1 indicate that the benefits are unlikely to be attributable to placebo effects.
Wilkins et al. (2001)52Study 1 evaluated 89 unselected children with IO and the WRRT on two sessions. The choice of colour was more repeatable than predicted by chance, although this could be explained by children remembering their initial choice. Those who were most consistent showed a tendency, which just reached significance, to manifest the greatest improvement in WRRT performance.
Study 3 investigated a new sample of 426 unselected children in 12 schools and investigated symptoms, WRRT performance, and sustained IO use nine months after IO testing. Thirty-one percent of the initial sample were still using an overlay after 9 months and these showed a significant tendency to be (1) the most symptomatic and (2) those who showed the greatest WRRT improvement on initial testing. Of the total sample, 5% read more than 25% more quickly with an overlay.
Although this paper cannot completely rule out placebo effects, the fact that colour was helpful but not grey (Study 2) and the sustained use for 9 months (Study 3) are suggestive of effects beyond those of a placebo.
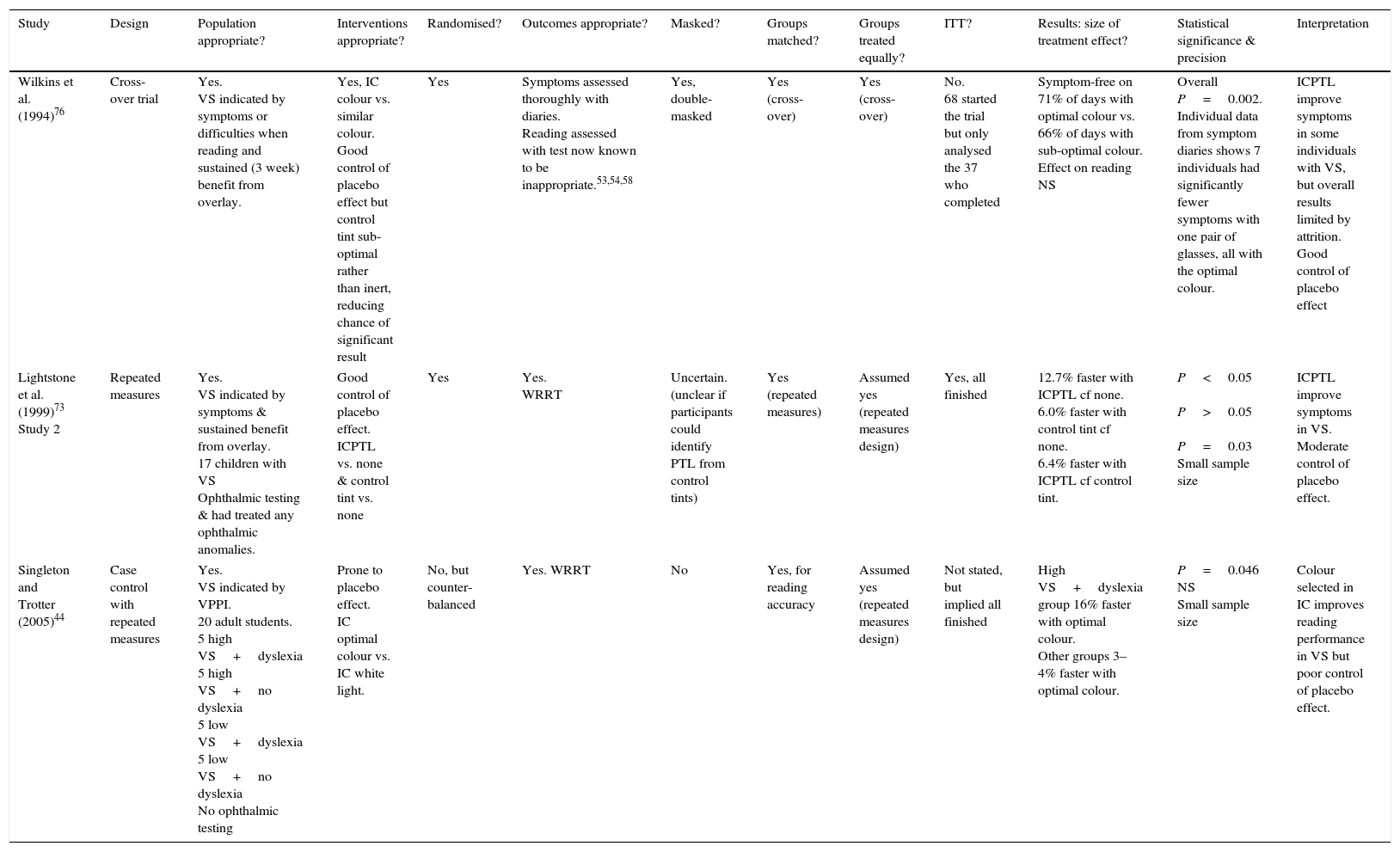
Controlled trials using the intuitive colorimeter (IC) and Precision Tinted LensesTable 3 evaluates all controlled trials of participants with VS using the IC. All studies found significant improvement of symptoms or performance from colour prescribed with the IC. All three studies and others16,17 support the notion that different individuals need different colours and the colour at least in some cases needs to be prescribed with a precision that is unlikely to be attributable to colour memory.16
Summary of controlled trials using intuitive colorimeter (IC) or Cerium Precision Tinted Lenses prescribed with the intuitive colorimeter (ICPTL) in populations selected as having VS. Abbreviations: ITT, intention to treat (were all of the participants who entered the trial properly accounted for at its conclusion?); NS, not significant; PGT, pattern glare test; VPPI, Visual Processing Problems Inventory (instrument with 24 questions relating to symptoms of VS); VST, visual search task; WPM, words per minute; WRRT, Wilkins Rate of Reading Test. Note 1: in these studies the WRRT was carried out as in recommended in the test instructions using an ABBA order to control for practice effects.52
| Study | Design | Population appropriate? | Interventions appropriate? | Randomised? | Outcomes appropriate? | Masked? | Groups matched? | Groups treated equally? | ITT? | Results: size of treatment effect? | Statistical significance & precision | Interpretation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wilkins et al. (1994)76 | Cross-over trial | Yes. VS indicated by symptoms or difficulties when reading and sustained (3 week) benefit from overlay. | Yes, IC colour vs. similar colour. Good control of placebo effect but control tint sub-optimal rather than inert, reducing chance of significant result | Yes | Symptoms assessed thoroughly with diaries. Reading assessed with test now known to be inappropriate.53,54,58 | Yes, double-masked | Yes (cross-over) | Yes (cross-over) | No. 68 started the trial but only analysed the 37 who completed | Symptom-free on 71% of days with optimal colour vs. 66% of days with sub-optimal colour. Effect on reading NS | Overall P=0.002. Individual data from symptom diaries shows 7 individuals had significantly fewer symptoms with one pair of glasses, all with the optimal colour. | ICPTL improve symptoms in some individuals with VS, but overall results limited by attrition. Good control of placebo effect |
| Lightstone et al. (1999)73 Study 2 | Repeated measures | Yes. VS indicated by symptoms & sustained benefit from overlay. 17 children with VS Ophthalmic testing & had treated any ophthalmic anomalies. | Good control of placebo effect. ICPTL vs. none & control tint vs. none | Yes | Yes. WRRT | Uncertain. (unclear if participants could identify PTL from control tints) | Yes (repeated measures) | Assumed yes (repeated measures design) | Yes, all finished | 12.7% faster with ICPTL cf none. 6.0% faster with control tint cf none. 6.4% faster with ICPTL cf control tint. | P<0.05 P>0.05 P=0.03 Small sample size | ICPTL improve symptoms in VS. Moderate control of placebo effect. |
| Singleton and Trotter (2005)44 | Case control with repeated measures | Yes. VS indicated by VPPI. 20 adult students. 5 high VS+dyslexia 5 high VS+no dyslexia 5 low VS+dyslexia 5 low VS+no dyslexia No ophthalmic testing | Prone to placebo effect. IC optimal colour vs. IC white light. | No, but counter-balanced | Yes. WRRT | No | Yes, for reading accuracy | Assumed yes (repeated measures design) | Not stated, but implied all finished | High VS+dyslexia group 16% faster with optimal colour. Other groups 3–4% faster with optimal colour. | P=0.046 NS Small sample size | Colour selected in IC improves reading performance in VS but poor control of placebo effect. |
The IC allows for placebo effects to be controlled because when colours are slowly adjusted in the IC colour adaptation causes participants to be unaware of the exact colour they are viewing. Thus, two colours can be selected which, according to the participant's reports, alleviate their symptoms to an optimal and sub-optimal degree without the participant being able subsequently to differentiate the appearance of each colour.76 The disadvantage of such a study is that the control tints are unlikely to be inert but rather are similar in colour to the optimal tint. If the two colours are made so similar that they are virtually identical then, although there will be a perfect placebo control, it would seem unlikely that the optimal colour will be sufficiently different to the sub-optimal colour for a difference in therapeutic effect to be evident. The research study using this approach included checks which confirmed that the trial was double-masked.76
The ability to detect a therapeutic effect can be improved by using symptom diaries, but this increases the risk of participant dropout, especially in a crossover study. This was a limitation of the research, since symptom diaries were completed for only 37 of the 68 participants who started the study (attrition bias). Also, the study was carried out before the WRRT was invented and therefore used a reading test that lacked the design characteristics required to show an immediate benefit from coloured filters in VS.53,54 This 20 year old study should be repeated with modern selection criteria,75 a larger sample, an appropriate reading test,53,54,58 and a proper implementation of the intention-to-treat principle.77 It is, however, notable that there were 7 participants who individually had significantly fewer symptoms with one pair of coloured lenses and in every case this was the lenses with the optimal colour, despite the fact that participants remained unaware throughout the study as to which pair contained the optimal colour.76
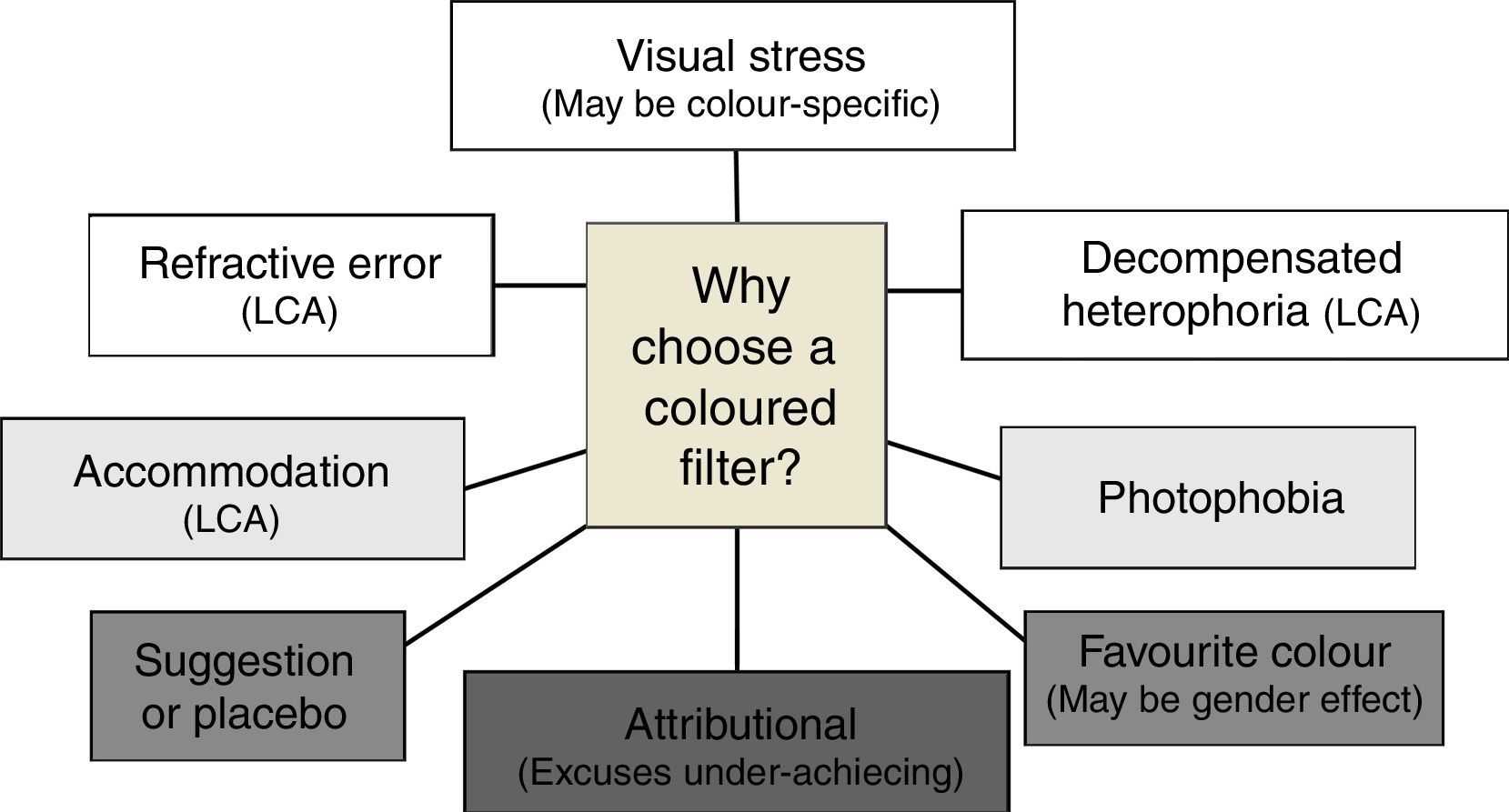
DiscussionOne factor contributing to conflicts in the literature is the heterogeneity of populations recruited to the various studies. IO11 and Cerium Precision Tinted Lenses78 were developed specifically to alleviate VS. There are three types of studies that are not included in this review because their selection criteria are unlikely to select samples of people with VS. First, in some studies recruitment strategies are based on participants experiencing reading difficulties or dyslexia,45,46 with only a relatively small percentage of these participants likely to experience VS. Second, some studies have investigated participants who have been prescribed coloured filters using the Irlen method, whose criteria are poorly stated and which can “detect” VS in close to 80% of people with reading difficulties.60 The present review also excludes studies where the sole selection criterion is that participants reported a preference for a coloured overlay, without any assessment of whether it improves performance or is used for a sustained period. This will over-diagnose VS, selecting about 50% of the population.12,51,52,54,57 There are a multitude of reasons why, on initial testing with overlays, children might choose a colour (see Fig. 2).

Requiring a trial with an overlay or an improvement in visual performance with the overlay will reduce the likelihood of a non-clinical reason for the improvement (dark grey panels in Fig. 2). Although the routine optometric examination gives little indication of visual stress,8 an eye examination should exclude clinical factors in Fig 2. Many of the symptoms experienced in visual stress are also typical in cases of uncorrected refractive error and accommodation-vergence anomalies and may disappear when these are corrected. Therefore, it is essential to conduct a full assessment of refractive status and binocular vision and to treat any anomalies conventionally before considering treatment with coloured filters. That said, anecdotal observations suggest that visual stress may exacerbate difficulties with accommodation and vergence and that these difficulties can sometimes be reduced when coloured filters are used. A positive result to a pattern glare test48,75,79 will further improve confidence in the diagnosis of VS.
Many studies in this review have only a limited control of the placebo effect. Colour adaptation means that the intuitive colorimeter can be used for a double-masked trial76 and a large RCT with this instrument is a priority for future research. Colour adaptation is also likely to explain why a person's optimal colour of overlay and lens will differ.73 These potential confounders are likely to increase the chance of a study finding that filters are helpful. In contrast, the tendency to over-diagnose VS in these studies59 reduces the likelihood of a positive result.
The diagnosis of VS needs further research. Few diagnostic processes have perfect sensitivity and specificity and inevitably in clinical practice there will be some individuals who are inappropriately diagnosed with a condition. This is clearly undesirable in clinical practice and will also reduce the statistical power of research studies. The authors have recently conducted a Dephi analysis which demonstrates some concordance in key tests in the diagnosis of VS but also a need for further research.75
Many of the papers in our review involved participants who had not received an eye examination to exclude other causes of symptoms. Although this diagnosis of exclusion is recommended for clinical practice,80,81 it is less important for research studies to apply this criterion because ophthalmic factors only infrequently account for symptoms of VS.8,55–57
In a recent review by Wilkins, a possible mechanism for VS has been elucidated that is related to a cortical hyperexcitability.26
Although beyond the scope of this review, the evidence for other visual factors (e.g., binocular instability) co-occurring with dyslexia is also modest,81 with a recent large study finding ophthalmic deficits in one in five children with severe reading impairment.82,83 Classroom learning requires clear and sustained vision and undetected visual problems may add to the burden that children with dyslexia or other learning difficulties experience. It would seem a sensible precaution for children who struggle at school to have an eye examination to exclude visual problems.84–88
The psychological effect of using coloured filters deserves consideration. In some children, they may play a positive role in helping them attribute underachievement to a condition rather than a lack of intelligence, but for others coloured filters may draw unwelcome attention. It is important for practitioners to appreciate that any interventions carry a cost to the patient and family in terms of expense, time, and raised expectations. For interventions where the evidence for the benefit is weak (e.g., coloured filters, small refractive errors, vision therapy) then the practitioner should be particularly careful not to overstate the case for intervening.
Despite the limitations of the research detailed above, the balance of evidence suggests that coloured filters can alleviate symptoms or improve performance in people who suffer from VS. The quality of evidence is less than would be required for new surgical or medical interventions, but coloured filters are a safer form of intervention. Until larger trials are completed, the authors recommend that before coloured lenses are prescribed practitioners should exclude other ophthalmic problems and assess the effect of overlays with the WRRT and a trial with overlays.
Contributors’ statementProfessor Evans and Professor Allen conceptualised and designed the study, performed the literature searches, drafted the initial manuscript, and approved the final manuscript as submitted.
Funding sourceNo external funding for this manuscript.
Financial disclosureThe authors have no financial interests in any coloured filter systems used to treat visual stress.
Conflicts of interestProfessor Evans has received honoraria for lectures and has acted as an expert witness on this topic. He is an unpaid committee member and secretary of the not-for-profit Society for Coloured Lens Prescribers (www.s4clp.org).
The following are the supplementary data to this article:





