

It has been reported that Kappa angle has an important role in laser refractive surgery procedures and implantation of multifocal intraocular lenses.1 The definition of Kappa angle in the literature is quite confusing because the same angle has been described by different names or the same term has been used to describe 2 different angles.2 Kappa angle is defined as the angle difference between the visual axis and pupillary axis. Visual axis is a theoretical axis defined as the line connecting the fixation point with the foveola, passing through the two nodal points of the eye.3 The pupillary axis can be determined locating a source such that the reflected image of this source (when viewed from the source) is centered on the entrance pupil (first Purkinje image over the pupil center).3 Although the Kappa angle is used commonly in literature, the Lambda angle is really measured as the angle between the pupillary axis and the line of sight, the latter defined as the line joining the fixation point and the pupil center.1,2 The reason why Kappa angle term can be used instead of Lambda angle is because visual axis and line of sight are nearly identical when the point of fixation is not very close to the pupil,4 thus it is commonly accepted to name Kappa angle as the angular difference between line of sight and pupillary axis.1,4
Corneal topographers are not centered over the line of sight but are centered over the first Purkinje image, which is the reflected image of the luminous fixation point from the anterior corneal surface also named vertex normal, topographer axis point, or coaxially sighted corneal light reflex if observer (topographer camera) views the eye along the same path as a light source.2,5 The distance from the center of the entrance pupil measured by the topographer and the light reflex is neither the lambda angle but it is the distance from vertex normal (topographer axis) to the corneal sighting center (line of sight).4,6 The pupillary axis therefore is not measured by corneal topographers and is more temporal to the light reflex and to the corneal sighting center (pupil center shown by the topographer).7
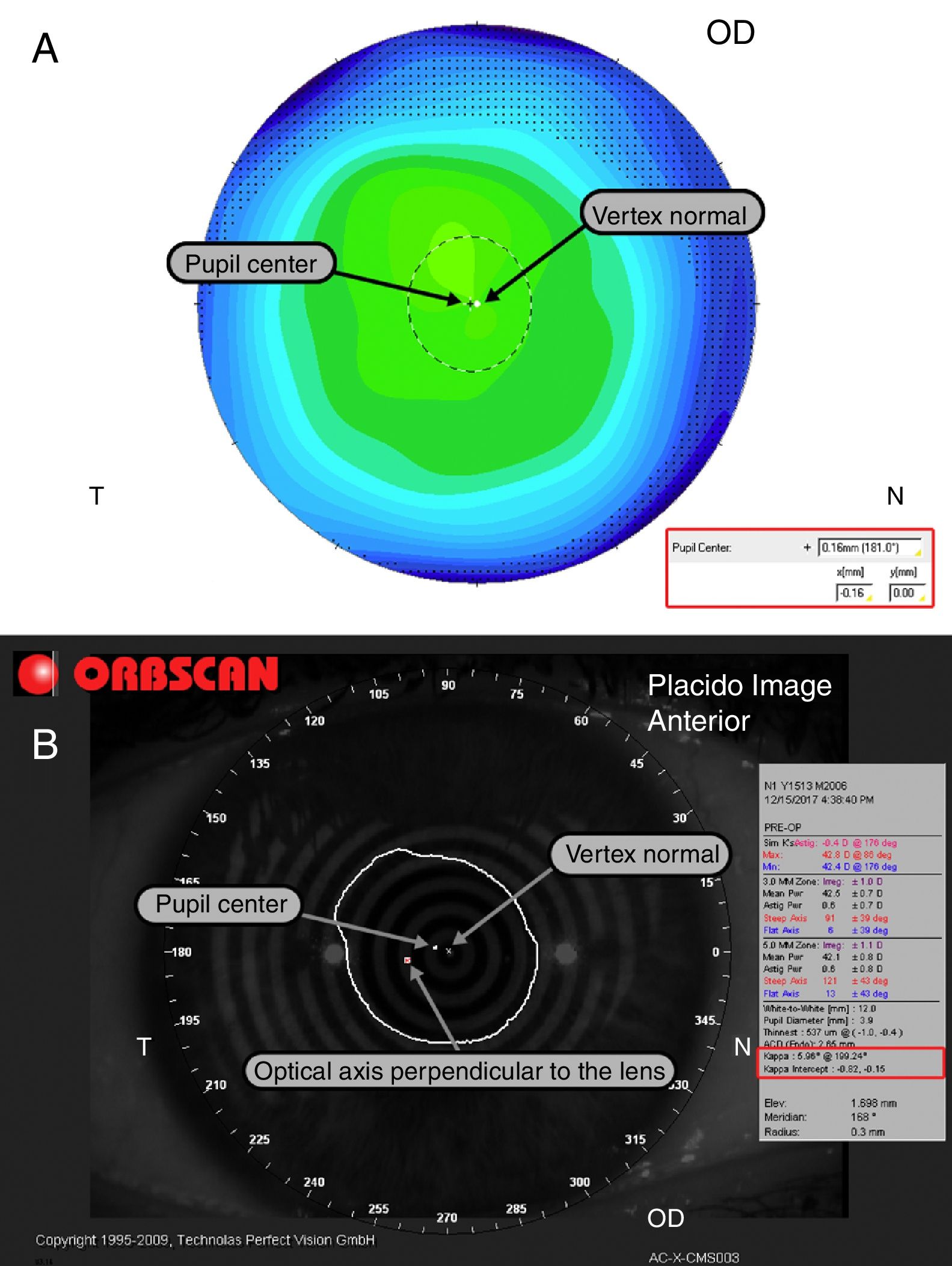
Early studies reporting Kappa angle with anterior segment devices were conducted with the Orbscan8 (Bausch & Lomb, Rochester, New York, USA) which defines the Kappa angle as the angle difference between the axis of fixation and the optical axis perpendicular to the lens.9 This definition neither correspond to the Kappa angle, but corresponds to the distance from optical axis of the lens and the first Purkinje image. Fig. 1 shows the same eye measured with Orbscan IIz (A) and Pentacam HR (B), while Orbscan describes the distance from the first Purkinje image to optical axis of the lens, Pentacam describes just the distance from the first Purkinje image to the pupil center (corneal sighting center or line of sight).
 and Pentacam (B). Orbscan reports Kappa angle as the distance from vertex normal to optical axis of the lens.")
Prakash et al.10 suggested that the occurrence of photic phenomenon was related to the Kappa angle measured with Orbscan after implantation of the multifocal intraocular lens. In our opinion, their conclusions should be interpreted with caution because the measure is not really the Kappa angle and previous studies reporting normal distribution of the angle from the Orbscan8 might not be transferable to other anterior segment devices. Anterior segment imaging devices do not report kappa angle but report a 2-dimensional Cartesian displacement that roughly correlates with the concept of kappa angle.2,6 Chang–Waring2 correctly addressed this issue and proposed the term chord mu (μ) or Chang–Waring chord11 in order to avoid the misunderstandings generated by the previous literature. Pentacam and other corneal topographers measure the chord mu defined as the distance from the pupil center (line of sight) to the light reflex (topographer axis). Care should be taken by the clinical researcher interpreting the names given by commercial devices because, as we pointed out, Orbscan Kappa angle does not comply with the definition of chord mu. Furthermore, other devices as the iTrace (Tracey Technologies, Houston, TX) use other angles as the alpha angle defined as the distance from vertex normal to center of white to white which is not really the alpha angle whose correct definition is the angle between the optical axis of the eye and the visual axis.3
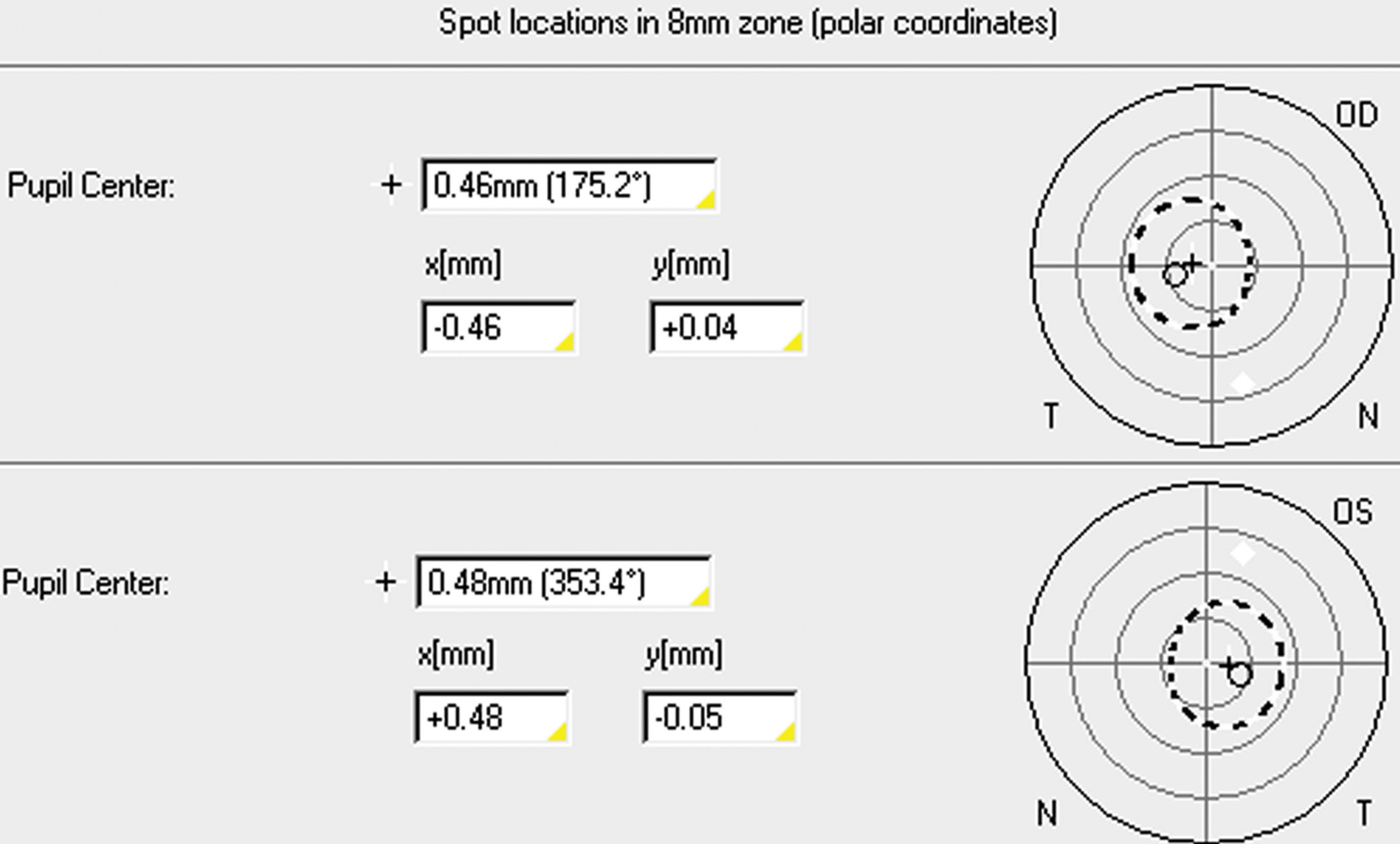
Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) is a Scheimpflug imaging device that reports the pupil center distance from the vertex normal as, as far as we know, commonly perform all the topographers. Therefore, it considers the vertex normal as the center of coordinates with negative values for indicating that the pupil is temporal or inferior to the light reflex in the right eye. Conversely, for the left eyes it uses positive values for indicating that the pupil is temporal and the same negative value for inferior location of the pupil center as it is shown in Fig. 2. Using the vertex normal as the center of coordinates might be confusing for the clinician because traditionally, the light reflex is evaluated considering the center of the pupil as the reference system in such a way that a positive angle is defined as the light reflex nasal to the pupil and a negative angle as the light reflex temporal to the pupil.8,12 If this is not specified in the research, the non-expert reader might be confused about the location of the light reflex, believing that it is normally located to temporal13 instead of nasal.14 In conclusion, Kappa angle is a term which should not be used with corneal topographers as Pentacam. The term chord mu should be used when reporting offset values between vertex normal and pupil center. Furthermore, a description shall be given as how interpret the values respect to the reference (vertex is reference or pupil is reference) and qualitative features (temporal/nasal, superior/inferior) because corneal topographers do not follow the historical nomenclature used in clinical practice. Special attention should be taken applying statistical analyses with data obtained from right and left eyes directly exported from corneal topographers because the coordinates system of one of the eyes should be flipped before combining all data. The combination of both eyes without applying this conversion can result in errors of interpretation.

No conflicting relationship exists for any author.





