

We tested the hypothesis that changes in accommodation after instillation of Phenylephrine Hydrochloride (PHCl) observed in some studies could be caused by changes in optics.
MethodsWe performed two experiments to test the effects of PHCl on static and on dynamic accommodation in 8 and 6 subjects, respectively. Objective wavefront measurements were recorded of the static accommodation response to a stimulus at different distances or dynamic accommodation response to a sinusoidally moving stimulus (between 1 and 3 D of accommodative demand at 0.2Hz). The responses were characterized using two methods: one that takes into account the mydriatic optical effects on the accommodation produced by higher-order aberrations of the eye and another that takes into account only power changes paraxially due to the action of the ciliary muscle and regardless of the pupil size.
ResultsWhen mydriatic optical effects were taken into account, differences in responses before and after PHCl instillation were 0.51±0.53 D, and 0.12±0.15, for static and dynamic accommodation, respectively, and were statistically significant (p<0.039). When mydriatic optical effects were not taken into account, the differences in responses before and after PHCl instillation were −0.20±0.51 D, and −0.05±0.14, for static and dynamic accommodation, respectively, and were not statistically significant (p>0.313).
ConclusionsThe mydriatic effect of the PHCl causes optical changes in the eye that can reduce the objective and subjective measurement of accommodation.
Probamos la hipótesis de que los cambios de la acomodación tras la instilación de Hidrocloruro de Fenilefrina (PHCl) observados en algunos estudios podrían estar originados por los cambios en la óptica.
MétodosRealizamos dos experimentos para probar los efectos de PHCl sobre la acomodación estática y dinámica en 8 y 6 sujetos, respectivamente. Se registraron las mediciones objetivas de frente de onda de la respuesta acomodativa estática a un estímulo a diferentes distancias, o la respuesta acomodativa dinámica a un estímulo con movimiento sinusoidal (entre 1 y 3 D de demanda acomodativa a 0,2Hz). Las respuestas se caracterizaron utilizando dos métodos: uno que tiene en cuenta los efectos ópticos midriáticos sobre la acomodación producida por aberraciones de alto orden, y otro que considera únicamente los cambios de potencia paraxialmente, debido a la acción del músculo ciliar, independientemente del tamaño de la pupila.
ResultadosAl tenerse en cuenta los efectos ópticos midriáticos, las diferencias de las respuestas antes y después de la instilación de PHCl fueron de 0,51±0,53 D, y 0,12±0,15, para la acomodación estática y dinámica, respectivamente, siendo estadísticamente significativas (p<0,039). Al no considerarse los efectos ópticos midriáticos, las diferencias en cuanto a las respuestas antes y después de la instilación de PHCl fueron de −0,2±0,51 D, y −0,05±0,14, para la acomodación estática y dinámica, respectivamente, no siendo estadísticamente significativas (p>0,313).
ConclusionesEl efecto midriático de PHCl origina cambios ópticos en el ojo que pueden reducir la medición objetiva y subjetiva de la acomodación.
Phenylephrine hydrochloride (PCHl) is a pharmacological agent usually used in the practice of ophthalmology to reinforce the mydriatic effect of other cycloplegic agents such as tropicamide.1,2 It can also be used alone to keep the pupil dilated while keeping active accommodation, which is useful in clinical evaluation of the accommodation mechanism.
As the iris dilator muscle controls pupil dilation, which is also influenced by the autonomic nervous system that innervates the ciliary muscle, miosis is typically presented during accommodation. The PCHl is often used alone in research studies of accommodation to disentangle its effects, e.g., increase in power, from other optical effects due to pupil changes, such as changes in depth of focus,3,4 change in aberrations and associated blur,5,6 or changes in retinal illumination.7,8
However complete isolation of the accommodation mechanism from pupil effects provided by the use of PHCl it is not frequently achieved. The possible effect that PHCl has on accommodation has been extensively studied, leading to conflicting, often contradictory, conclusions.9 Numerous studies concluded that there is some loss in accommodation after PHCl instillation,10–14 even if the reduction in accommodative performance is modest and does not carry a large clinical significance.15 Others concluded that accommodation is unaffected.1,16 Yet others concluded that dynamic accommodation (accommodation response to a moving stimulus) but not static accommodation is affected by PHCl instillations.1,16–19
We hypothesize here that PHCl does not have a cycloplegic effect, but rather the observed losses in accommodation ability are due to secondary optical factors associated with its mydriatic effect.
Materials and methodsTo test the hypothesis that PHCl does not have a cycloplegic effect, we carried out two independent experiments. In the first experiment, we calculated the accommodative responses to stimuli at different distances. In the second experiment, we calculated the accommodative responses to a moving target that changed optical vergence sinusoidally. Each experiment was repeated twice: first before instillation of PHCl and then after instillation of PHCl. The accommodative responses to both the first, static accommodation experiment, and the second, dynamic accommodation experiment, were obtained from objective wavefront measurements using two different metrics. The first metric takes into account the change in power during accommodation produced by rays passing through the whole pupil (Zernike refraction20). The second metric takes into account the change in power produced by rays passing through the central part of the pupil (paraxial or Seidel refraction20). The latter method to calculate the accommodative response of the eye is only affected by the change produced by the action of the ciliary muscle, whereas the former method is affected by change in the ciliary muscle and change in higher-order aberrations (HOAs), in particular the presence of spherical aberration. Both methods to obtain the state of accommodation of the eye are described in more detail in Section Data analysis.
SubjectsAll the subjects involved in the static and dynamic accommodation experiments were healthy participants. None of them had astigmatism greater than 1 D. Their best-corrected visual acuity was at least 20/20 in Snellen equivalent. The subjects had no ocular abnormality or systemic condition, no history of ocular surgery, and presented clear intraocular media. The study adhered to the tenets of the Declaration of Helsinki and all participants gave written informed consent before participating in the study. The Ethics Committee approval was obtained.
Ten healthy participants took part in the study of static accommodation. Two of them were removed due to the fact that the PHCl did not seem to have any effect on them, as their pupil size did not show any change. This lack of effect could be due to differences in iris pigmentation or other factors not controlled in the experiment. The mean spherical equivalent among the eight remaining participants was −0.23 ± 1.21 D and their mean age was 25 ± 6 years, ranging from 21 to 38 years. Five participants were female and three were male.
Seven healthy subjects participated in the dynamic-accommodation study. One of them was removed due to the fact that its refraction changed more than 1 D after instilling the PHCl. The mean spherical equivalent among the six remaining participants was −0.17 ± 2.08 D and their mean age was 33 ± 6 years, ranging from 26 to 39 years. Two participants were female and four were male. Amplitude of accommodation (AA) of the subjects who participated in the dynamic accommodation study was known to be larger than 3 D from previous experiments.
Experimental procedureStatic and dynamic measurements of accommodation were recorded monocularly under normal conditions, and at least 30minutes after the instillation of two drops of 10% PHCl. Drops were administered to the subjects within a 5-minute interval before the trials. Measurements started once the PHCl had its effect. Participants were told to make the same effort clearing the target as if they were reading a book and were allowed to rest between trials as required.
For static accommodation, measurements were obtained using the irx3 commercial aberrometer (Imagine Eyes, Orsay, France). The irx3 aberrometer has a Hartmann-Shack wavefront sensor, a polychromatic target with low and high spatial frequency content, and a Badal optical system that allows measurement of aberrations while the eye is accommodating. Three typical stimulus-response curves were measured monocularly for each participant by approaching the stimulus discretely in steps of 0.5 D and starting 1 D further away from their far point to avoid over-accommodation. From the three curves, the one that showed the largest AA (assumed as the maximum minus minimum of the full accommodative response) was selected for each participant. Further details of the measurements can be seen elsewhere.21,22
For dynamic monocular accommodation, a custom-made adaptive optics system was used to carry out the measurements. It includes a Hartmann-Shack wavefront sensor, a deformable mirror, a Badal optical system, used to compensate the subject's spherical equivalent and change the stimulus vergence, a white microdisplay for presenting the stimulus target (Maltese cross, with 20cd/m2 and spanning 1.95 degrees of visual angle), and an artificial pupil of 3mm in diameter. Further details of the system can be obtained elsewhere.23
First, the subjective far point for each subject was measured three times using the Badal system. For the dynamic measurements of accommodation, the Badal system was used to change the vergence of the target sinusoidally at 0.2Hz between 1 and 3 D of accommodative demand with respect to the refractive state of each subject, during trials lasting 25seconds. Subject's aberrations were measured at 10Hz. This procedure was repeated six times.
Data analysisWavefront aberrations obtained with and without PHCl at different stimulus vergences were expressed in Zernike coefficients of an expansion up to the 8th order. Refractive state was then calculated using two different wavefront refraction24 methods that have been widely used for this purpose.20,25 The first method, minimum root mean square (RMS) or Zernike refraction,20,26 takes into account the refractive change produced at different parts of the pupil. The second method, commonly known as paraxial or Seidel refraction,20,26 only takes into account the refractive power change that takes place in a small central part of the optics of the eye. Mathematically, the main difference between these two metrics is the presence of spherical aberration in the eye. When no spherical aberration is presented, both metrics shows the same results.20,24
The use of these two metrics allows us to differentiate the refractive changes produced by the action of the ciliary muscle in the lens (paraxial refraction) from the refraction that also takes into account the optical effects that originate from minimum RMS refraction.
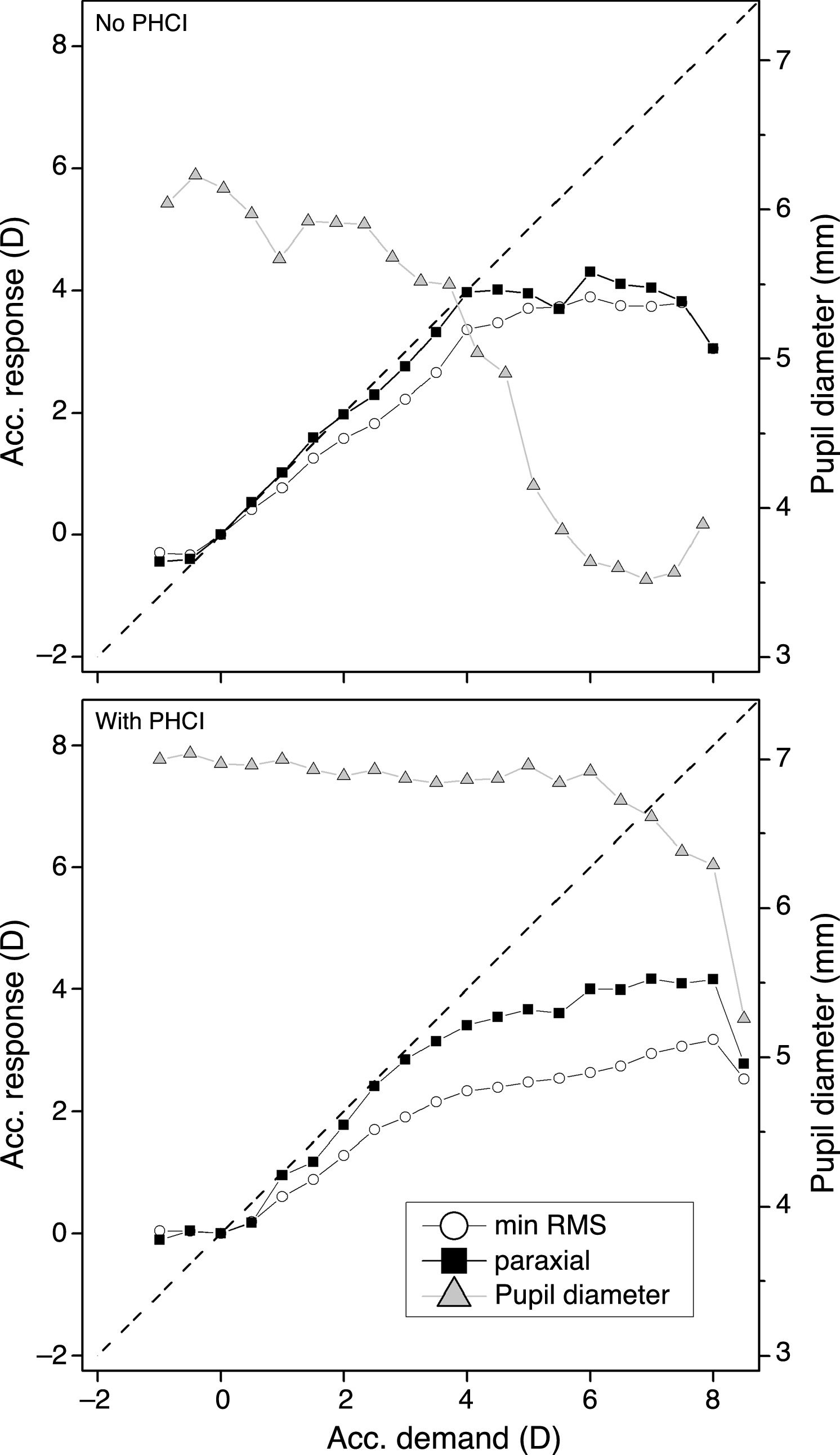
For the static measurements, in addition to the AA, the accommodative response (AR) was also obtained for 6 D of accommodative demand since that was the accommodative demand where the pupil size of the some subjects started to close down when PHCl was applied (see Fig. 1). Sometimes, when the measured pupil diameter without PHCl was very small (less than 3mm) and the eye was close to the near point in accommodation, unusual values of aberrations were obtained. These clear outliers were removed manually from the curve prior to the calculation of AA. No data points were removed in the calculation of the accommodative response at 6 D.

Stimulus-response curves obtained from a typical subject for the two calculation methods, minimum RMS refraction and paraxial refraction. Top panel shows the curve before PHCl instillation. The bottom panel shows the curve after PHCl instillation. Dashed black line represents the ideal response.
For the dynamic measurements, a sinusoidal function with the same frequency, 0.2Hz, as the accommodative demand and with two parameters, amplitude in D and temporal phase in seconds, was fitted to the accommodative response over time. The gain of the accommodative response was then calculated as the amplitude of accommodative response over the amplitude accommodative demand.22 The temporal phase gives information about the difference in time between the response and the demand; that is, the time lag of the response with respect to the demand (see reference23 for further details).
For the static measurements, changes in AA and AR for an accommodative demand of 6 D before and after instillation of PHCl were assessed. Likewise, changes in gain and phase between responses before and after instillation of PHCl were assessed. Prior to this analysis, normality of the data was checked using the Shapiro-Wilk method. Since part of the data did not follow a normal distribution, the non-parametric Wilcoxon signed-rank test was used. A significance level of 0.05 was used when comparing any accommodation result in our study.
ResultsStatic measurements of accommodationFigure 1 shows the stimulus-response curves obtained from a typical subject with and without the instillation of PHCl as calculated with minimum RMS refraction and paraxial refraction.
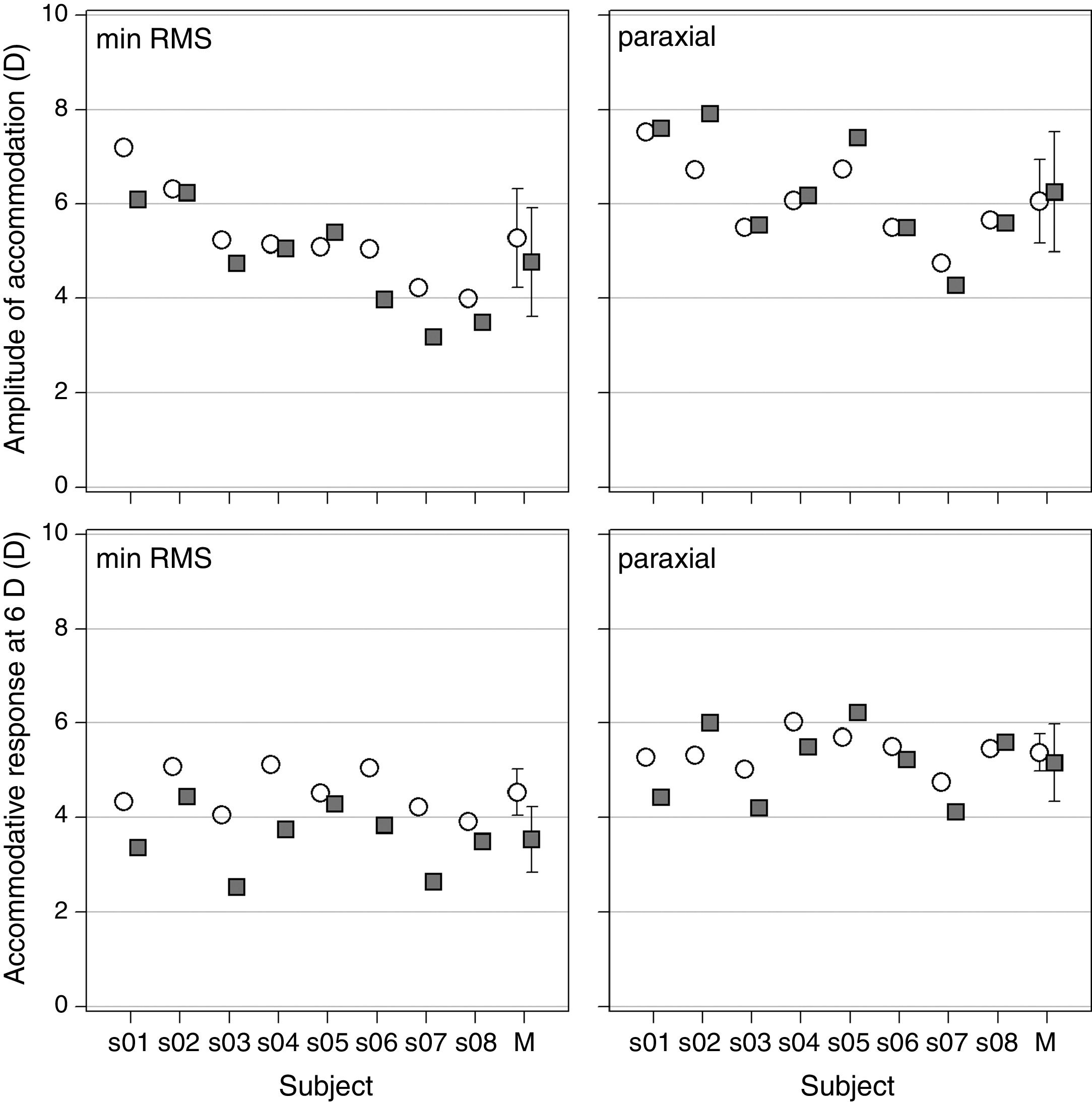
The AA of each participant calculated with both metrics is displayed in the upper panel of Figure 2. The lower panel of Figure 2 shows response at 6D of accommodation demand calculated with the minimum RMS refraction (left panel) and with the paraxial refraction (right panel).
 or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Lower row shows the calculated response at an accommodative demand of 6 D. Empty circles stand for the natural condition, whereas filled squares show results after instillation of PHCl. Error bars in the mean represent one standard deviation. M stands for the mean over subjects.")
Static accommodation results. Upper row shows the AA for each subject when the minimum RMS refraction (left panel) or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Lower row shows the calculated response at an accommodative demand of 6 D. Empty circles stand for the natural condition, whereas filled squares show results after instillation of PHCl. Error bars in the mean represent one standard deviation. M stands for the mean over subjects.
The mean difference in AA before and after PHCl instillation over subjects was 0.51 ± 0.53 D (p = 0.039) when calculated with the minimum RMS refraction, while the paraxial refraction yielded a difference of −0.20 ± 0.51 D (p = 0.313). The Wilcoxon signed-rank test showed significant differences between before and after instillation of PHCl when the minimum RMS refraction was used, whereas it did not show significant differences when the paraxial refraction was used. For the response at 6 D of accommodative demand, the mean difference was 1.00 ± 0.51 D (p = 0.008) and 0.22 ± 0.60 D (p = 0.313). when calculated for minimum RMS refraction and paraxial refraction, respectively. In this case, the Wilcoxon signed-rank test showed significant differences when minimum RMS refraction was used for the computation of the response; however, no differences were found with the paraxial refraction.
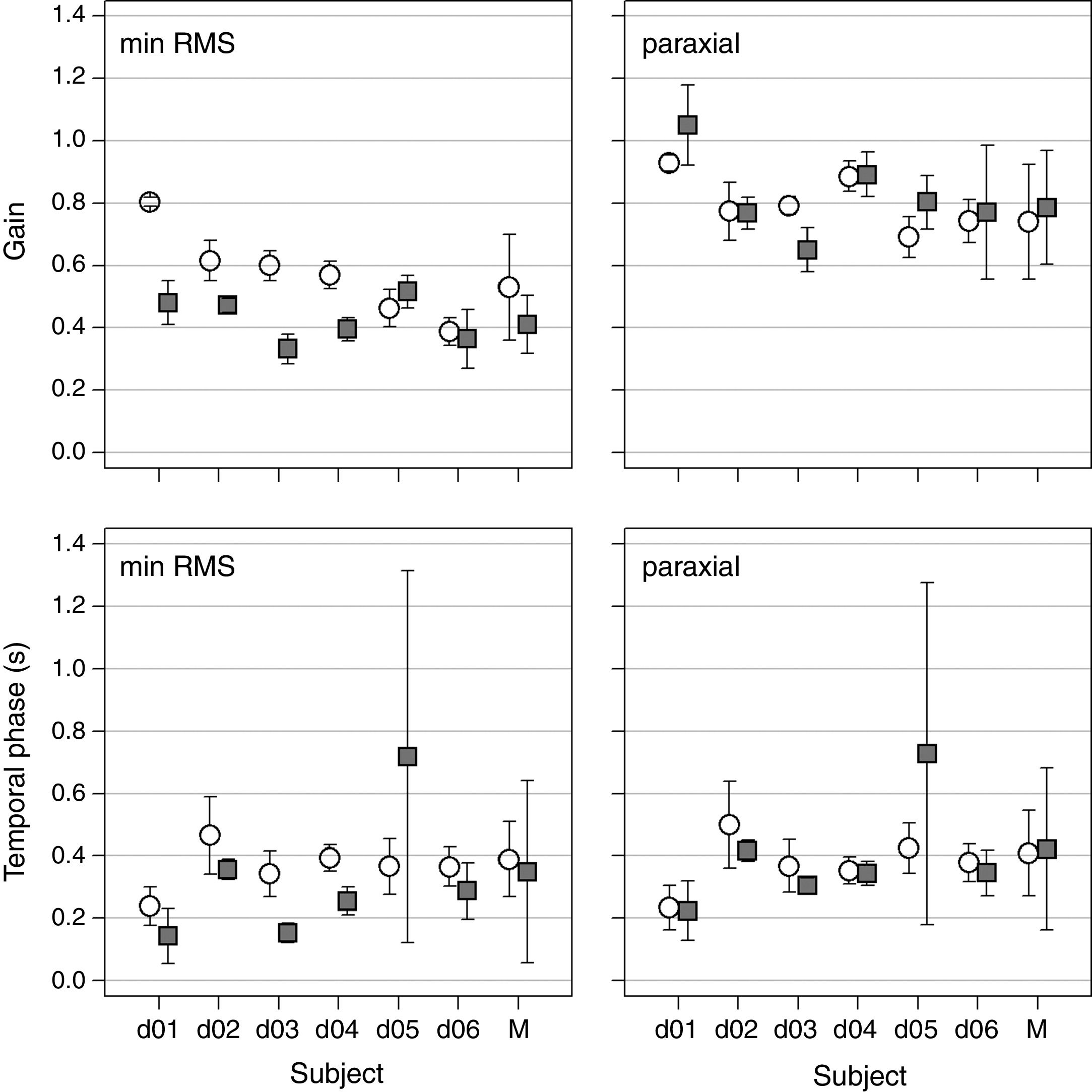
Dynamic measurements of accommodationThe upper and lower panels in Figure 3 show the mean gain and temporal phase (with corresponding standard deviations) obtained for each subject when both the minimum RMS refraction (left) and the paraxial refraction (right) were used to calculate the accommodative response.
 or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Lower row displays the mean phase in seconds for each subject when the minimum RMS refraction (left panel) or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Error bars represent one standard deviation among the six trials for each subject. Other details as in Figure 2.")
Dynamic accommodation results. Upper row shows the mean gain for each subject when the minimum RMS refraction (left panel) or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Lower row displays the mean phase in seconds for each subject when the minimum RMS refraction (left panel) or the paraxial refraction (right panel) was applied for the computation of the accommodative response. Error bars represent one standard deviation among the six trials for each subject. Other details as in Figure 2.
Mean difference in gain computed for the minimum RMS refraction were 0.12 ± 0.15 (p<0.001), while in paraxial refraction where −0.05 ± 0.14 (p=0.360). Generally, paraxial refraction yielded greater values of gain than the minimum RMS refraction. With the paraxial refraction, all the subjects except one showed practically the same gain or greater gain after instillation of PHCl.
Except for one subject, for the minimum RMS refraction, temporal phase was similar but systematically greater before instillation of PHCl. The mean temporal phase difference was 0.04 ± 0.30seconds (p<0.001). For paraxial refraction, there were no systematic differences, with mean temporal phase difference of −0.01 ± 0.26seconds (p=0.160). The Wilcoxon signed-rank test gave statistically significant differences for the minimum RMS refraction, but not for the paraxial refraction.
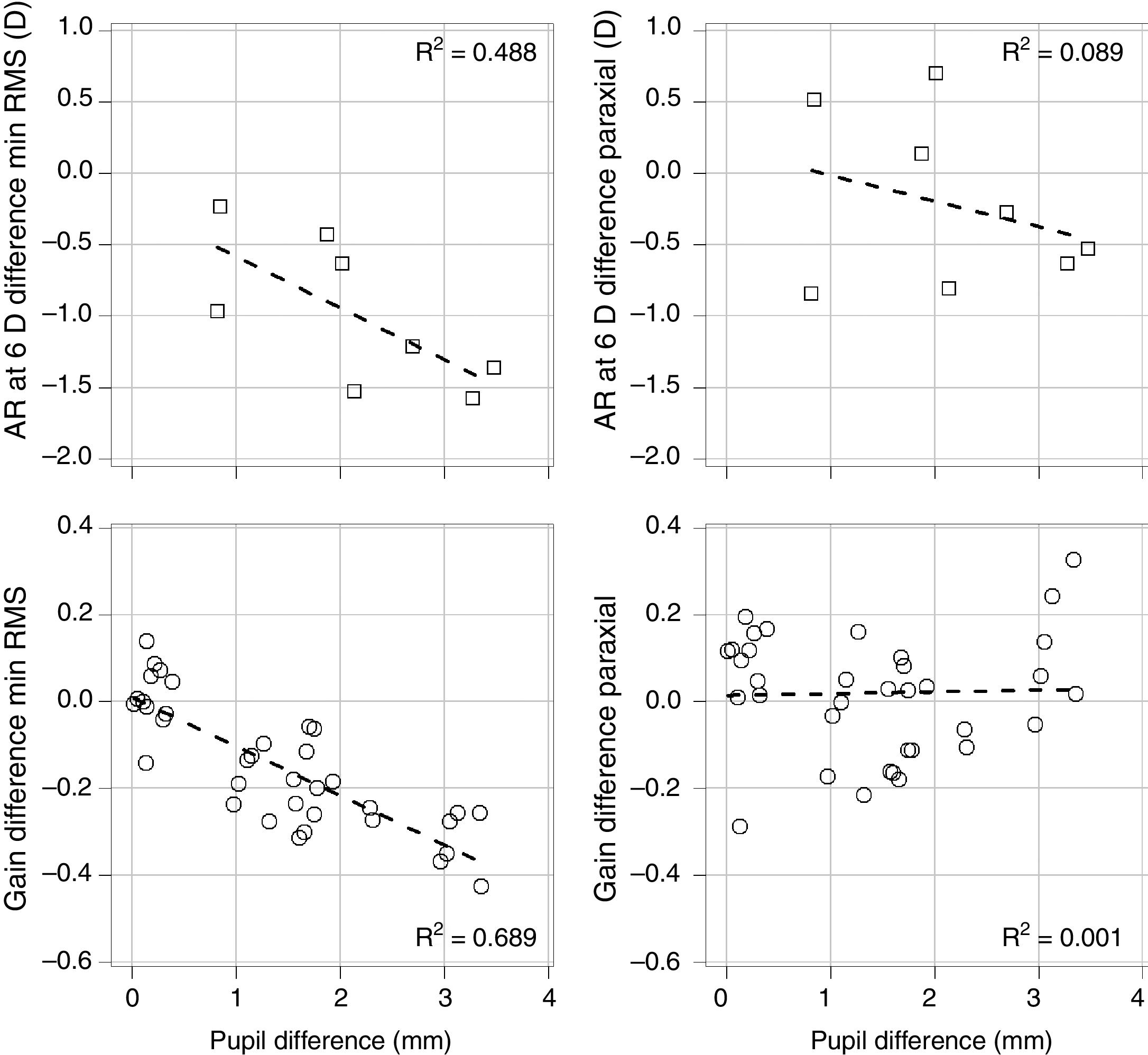
Comparison between metricsThe upper panel of Figure 4 shows the relationship between the differences in response at 6 D of accommodation demand with and without PHCl with respect to the differences in pupil size measured at the same demand, for the two metrics used in this study: minimum RMS refraction (left) and paraxial refraction (right). The lower panel of Figure 4 shows the relationship between the differences in gain obtained with and without PHCl in the dynamic accommodation, with respect to the differences in averaged pupil size throughout the trials.
 and the paraxial refraction (right column). The upper row shows static accommodation. The lower row shows the gain obtained for each trial and subject (6 trials and 6 subjects) with respect to the difference in averaged pupil size throughout the trials for the dynamic accommodation. The dashed line represents the best linear fit to the data. The coefficient of determination (R2) obtained in each case is displayed.")
Accommodation and pupil size. Relationship between the differences in gain after and before instillation of PHCl as a function of the differences between pupil sizes, for the minimum RMS refraction (left column) and the paraxial refraction (right column). The upper row shows static accommodation. The lower row shows the gain obtained for each trial and subject (6 trials and 6 subjects) with respect to the difference in averaged pupil size throughout the trials for the dynamic accommodation. The dashed line represents the best linear fit to the data. The coefficient of determination (R2) obtained in each case is displayed.
Figure 4 shows that, in any case, for the minimum RMS refraction, a greater difference in pupil sizes is accompanied by a greater difference between responses, whereas for the paraxial refraction, the differences between responses cannot be explained by differences in pupil sizes. This result outlines the effect that pupil size has on accommodation calculated by both metrics.
DiscussionIndependent studies on the effect of PHCl on accommodative ability of the ciliary muscle have reported contradictory results.9 These studies were based on measuring the subjective perception of blur, the objective refractive state of the eye, or by means of indirect (non-optical) measurements. Our results shed light into this controversy, by showing that the observed effect of PHCl on the function of the ciliary muscle is highly dependent on the way the accommodative response is calculated. Based on our results here and of those in previous reports,10,15 PHCl does not seem to affect the ciliary muscle.
This study was designed so that each subject had repeated measurements, before and after PHCl instillation. It departs from standard clinical trials where a treatment group is compared against a control group. From a clinical viewpoint, we could describe this study as a type of self-controlled case series,27 since subjects under normal conditions (control) are compared against themselves after instillation of PCHI conditions (treatment).
Our results demonstrate that differences in the accommodative ability after the instillation of PHCl or lack thereof depends on the method to calculate the accommodative response. When HOAs were taken into account (minimum RMS refraction), there were significant differences before and after instillation of PHCl for both static and dynamic accommodation. However, when only the change of the unbalanced defocus (paraxial refraction) was used to calculate response, accommodation before and after the instillation of PHCl was similar and not significantly different.
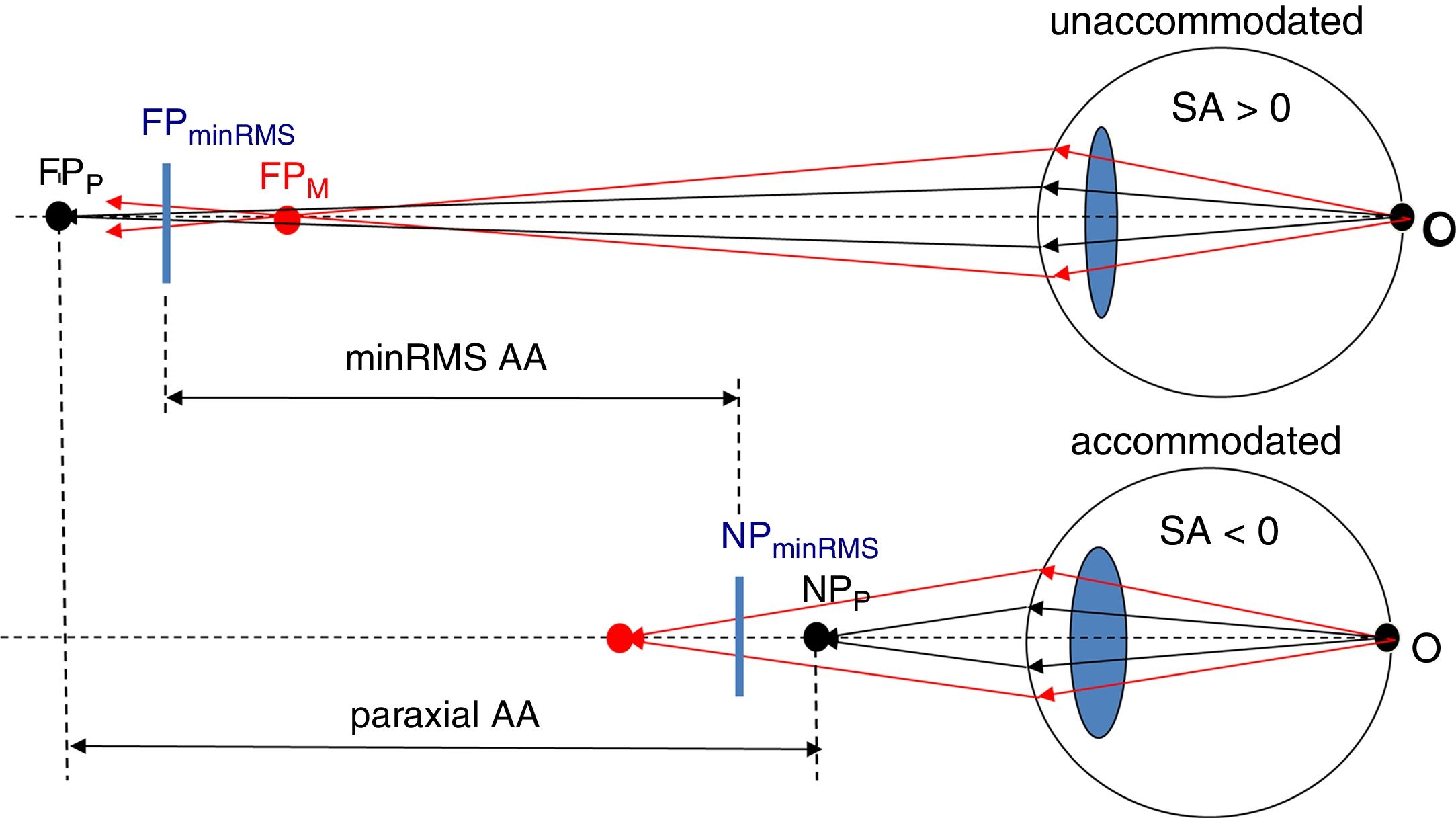
Previous studies have found that fourth-order Zernike spherical aberration and its change from a positive to a negative value during accommodation,22,28,29 has an impact in the accommodation response obtained objectively28 as well as in the AA obtained subjectively.30Fig. 5 illustrates this impact schematically.
. Minimum RMS AA is represented by the distance between an intermediate position of the distance of the paraxial (FPP and NPP) and the marginal (FPM and NPM) far and near points, FPminRMS and NPminRMS, respectively. Paraxial and marginal points exchange their relative distance to the eye after accommodation because the spherical aberration changes it sign. Note the effect of SA on accommodation by comparing Paraxial AA (not affected by SA) with minRMS AA (affected by AA).")
Effect of spherical aberration on the AA. Paraxial AA represents the vergence distance between the far and near points when using paraxial rays (black rays). Minimum RMS AA is represented by the distance between an intermediate position of the distance of the paraxial (FPP and NPP) and the marginal (FPM and NPM) far and near points, FPminRMS and NPminRMS, respectively. Paraxial and marginal points exchange their relative distance to the eye after accommodation because the spherical aberration changes it sign. Note the effect of SA on accommodation by comparing Paraxial AA (not affected by SA) with minRMS AA (affected by AA).
If an optical system measures the refraction of an eye under cycloplegia using minimum RMS refraction, which is equivalent to the system looking for maximum intensity of the image of a point source on the retina,31 such as many autorefractometers, or similar to the use of retinoscopy,32 the accommodation or the AA will depend on the image formed by rays passing through the whole pupil. Then, accommodation will be smaller than measurements obtained when only paraxial rays are taken into account (black rays in Fig. 5). Paraxial rays are insensitive to mydriatic effects of the PHCl, and the refraction will only depend on the central power changes of the crystalline lens. Subjective refraction is also affected slightly by the effects of spherical aberration, so when the rays travel from the object to the retina, a similar effect will be found.30
Spherical aberration becoming more negative when accommodation increases can also explain the reason of obtaining large values of lag when determining the accommodation response with the minimum RMS refraction (see bottom left panel in Fig. 2). As a consequence, subjects could tolerate greater lags in accommodation because the tolerance is larger to negative defocus.31
In our results, mean gain obtained with the paraxial refraction after PHCl instillation increased for 4 out of 6 subjects, remained stable for 1 subject, and decreased for another subject.
ConclusionWe give an optical explanation to the fact that many authors have found a decrease in objective measurements of the static and dynamic accommodation after PHCl instillation. The explanation is based on the presence of larger values of spherical aberration in the mydriatic eye, its change during accommodation and its influence on the subjective and objective measurement of the accommodation. Even though our study is based on a relatively small population, it shows clear results and should be taken into account in future works where PHCl is used on studies related to static and dynamic accommodation. Future studies about the effect of PHCl on accommodation should be carried out obtaining the accommodation response in a small pupil area; that is, using paraxial refraction.
FundingThis work was supported by the European Research Council [Starting Grant ERC-2012-StG-309416]; and the University of Valencia [UV-INV-PREDOC14-179135].
Conflicts of interestThe authors have no conflicts of interest to declare.





